|
|
Part
I Spousal
and Partner Abuse |
2008
If
you are in danger call 911 or |
| This course provides a comprehensive overview of domestic violence, details numerous research studies and findings from state and local domestic violence programs, and reviews case experiences of advocates who work with victims and batterers. Protocols and policies for criminal justice system, legal, and coordinated community-based interventions are also examined, along with summaries of federal and state laws relevant to domestic violence prevention and interventions. Aspects of the physical, psychological, and financial impact of domestic violence on its victims, and on children who witness violence, are addressed. |
Around
the world at least one woman in every three has been
beaten, coerced into sex, or otherwise abused in her
lifetime. Most often the abuser is a member of her own
family. Ending violence against women, a report from the Center for Communications Programs, Johns Hopkins University |
Approximately
1.5 million women and 834,700 men are raped and/or
physicallyÊassaulted
by an intimate partner each year. Center for Disease Control |
Children
who witness domestic violence are more likely to exhibit
behavioral and physical health problems including depression,
anxiety and violence towards peers. Adolescents are also
more likely to attempt suicide, abuse drugs and alcohol,
run away from home, engage in teenage prostitution and
commit sexual assault crimes. U.S. Department of Health & Human Services |
| More
women than men experience intimate partner violence. According
to the National Violence Against Women Survey, 1 out of 4
U.S. women has been physically assaulted or raped by an intimate
partner; 1 out of every 14 U.S. men reported such an experience Center for Disease Control |
This
15 unit course
addresses the
'red flags'
assessment,
detection, and
intervention strategies including
community resources,
cultural factors,
substance abuse,
same gender abuse dynamics, and
treatment regarding
spousal or partner
abuse
and may be taken in fulfillment of the ![]() CA
BBS and BOP mandated continuing abuse requirement
CA
BBS and BOP mandated continuing abuse requirement
Increasingly,
gender-based violence is recognized as a major public health concern
and a violation of human rights. The effects of violence can be
devastating to a woman's reproductive health as well as to other
aspects of her physical and mental well-being. In addition to
causing injury, violence increases women's long-term risk of a
number of other health problems, including chronic pain, physical
disability, drug and alcohol abuse, and depression. Women with
a history of physical or sexual abuse are also at increased risk
for unintended pregnancy, sexually transmitted infections, and
adverse pregnancy outcomes. Yet victims of violence who seek care
from health professionals often have needs that providers do not
recognize, do not ask about, and do not know how to address."(Ending
violence against women, a report from the Center for Communications
Programs, Johns Hopkins University at http://www.infoforhealth.org/pr/l11edsum.shtml)Volume
XXVII, Number 4
December, 1999
Series L, Number 11
Issues in World Health
The best way to uncover a history of abuse in female clients is
to ask about it. Nonetheless, several types of physical injuries, health
conditions, and client behavior should raise health care providers' suspicion
of domestic violence or sexual abuse. When these signs, or 'red flags,'
are present, providers should be sure to ask their clients about possible
abuse, remembering to be empathic and respectful of the client's privacy.
| Chronic, vague complaints that have no obvious physical cause, | Pregnancy of unmarried girls under age 14, | ||
| Injuries that do not match the explanation of how they occurred, | Sexually transmitted infections in children or young girls, | ||
| A male partner who is overly attentive, controlling, or unwilling to leave the woman's side, | Vaginal itching or bleeding, | ||
| Physical injury during pregnancy, | Painful defecation or painful urination, | ||
| Late entry into prenatal care, | Abdominal or pelvic pain, | ||
| A history of attempted suicide or suicidal thoughts, | Sexual problems, lack of pleasure, | ||
| Delays between injuries and seeking treatment, | Vaginismus (spasms of the muscles around the opening of the vagina), | ||
| Urinary tract infection, | Sleeping problems, | ||
| Chronic irritable bowel syndrome, | A history of chronic, unexplained physical symptoms, | ||
| Chronic pelvic pain. | Having difficulty with or avoiding pelvic exams, | ||
| Problems with alcohol and drugs, | |||
| Sexual 'acting out,' | |||
| Extreme obesity. | |||
Fuente: Center for Health and Gender Equity y Family Violence Prevention Fund (460). |
|||
source: http://www.infoforhealth.org/pr/l11/l11pullout.shtml#top
What
are the warning signs of an abusive spouse or partner?
According to the National Coalition Against Domestic Violence, the following
signs are common predictors of abuse:
violent family life;
use of violence or force to "solve" problems;
use of alcohol or other drugs;
strong traditional ideas about the role of husband and wife;
jealousy of a spouse or partner's other relationships;access to weapons, such as knives or guns, and threats to use them;
expectation that a spouse or partner will follow orders or advice;
mood swings with extreme highs and lows;
rough treatment of a spouse or partner
http://www.mentalhealth.org/highlights/october2003/domestic/
Please go to: Potential Problems for Psychologists Working with the Area of Interpersonal Violence
While this article is written specifically for psychologists, it has important information about the dangers of working with spousal and partner abuse for all mental health professionals.
"Interpersonal violence cases have the potential for the most dangerous outcomes. It is important for psychologists in their various roles to ensure safety, prevent harm whenever possible (General Principle E, F, and ES 1.14), and to warn clients or others in danger. In all interpersonal violence cases or alleged cases, it is crucial that some type of assessment of the abuse or violence be conducted, and the risk of harm be ascertained. It is also important that all clinical cases be evaluated or screened to determine the likelihood of present or past abuse or violence....
Psychologists should have an up-to-date awareness of the ethical and legal standards that affect their practice. Knowledge of confidentiality and exceptions to confidentiality is particularly important when working with clients who may be involved with violence." Please go to APAonline for the complete article at http://www.apa.org/pi/pii/professional.html?CFID=2636885&CFTOKEN=52026085
California
psychologists please go to: http://www.psychceu.com/ca-bop_law_summary.pdf
for State Of California Department Of Consumer Affairs Board Of Psychology Summary
Of California Laws Relating To The Practice Of Psychology.
![]()
You may need to
get Adobe Acrobat to view this and other pdfs; please go to http://www.adobe.com/products/acrobat/readstep2_allversions.html
.
"Licensed Marriage and Family Therapists are not mandated reporters
of domestic violence. If an LMFT reports domestic
violence, it is a breach of confidentiality, regardless of the
work setting or employer. As reported in the November/December 1994
issue of The California Therapist, LMFTs are not to report domestic
violence, even though there still seems to be confusion about this subject
in practice.
California Penal Code §1160(a) states that a health practitioner
who is providing medical services for a physical condition is a mandated
reporter. LMFTs do not provide services for physical conditions. Therefore,
LMFTs do not report domestic violence. There is no exception for LMFTs
in settings where physical health treatment is provided. There is no
exception for LMFTs even if your employer has a different policy. No
local policy of any agency or county takes precedence over state law."
(Pelchat, Z., "LMFTs Do Not Report Domestic Violence", January/February 2001, The California Therapist)
Confusion -Do you report Spousal or Partner abuse if the patient is an elder, as Elder Abuse is mandated for reporting in California? For more information, please go to ADULT PROTECTIVE SERVICES MANDATED REPORTERS . (In this situation, I would call the free legal counsel available through my professional organization.)
"the right to privacy ends where the public peril begins" and that "clear and immediate probability of physical harm" to others allows for the breaking of confidentiality.
"There
are six pieces that must be documented when a patient makes a serious
threat of violence before a Tarasoff warning is indicated. They are:
1. a patient
2. tells
3. you, the therapist (or your psychological assistant)
4. a serious threat
5. of physical violence
6. against a reasonably identifiable victim
The consequences of not following the 'duty to warn' include liability,
as you may be held responsible for any harm done, not only to the intended
victim, but any others who are injured when the patient tries to harm
the intended victim.
Document everything if you are going to invoke Tarasoff. This includes
the stated threat, the means to carry it out, your attempts to locate
the intended victim, as well as notifying the appropriate law enforcement."
(Pelchat, Z.,
"Tarasoff for Clinicians: A User's Guide to the Law", November/December
2001, The California Therapist)
For more on this, go to "Summary of Final Rule Providing Standards
for the Privacy of Patient Records", at APAonline, at
http://www.apa.org/practice/medrecsum.html
As
the laws are different for each state and license, you
MUST know what the legal and ethical obligations are for you,
in your state, with your license.
Please go now and do a search for your state and license. (We will
ask you for this information on the post-test.) Go to http://www.feminist.org/911/crisis.html as
they have links for each state.
(If you do not know how to search, we recommend Google. Just put in the relevant words, such as LCSW mandated reporter domestic violence MA; you will get a page of links. See if you can find the answer. An example is:
For Massachusetts Social Workers, this information was found at: The National Association of Social Workers - Massachusetts Chapter:
The NASW Code of Ethics Applied: Confidentiality at http://www.naswma.org/content.asp?contentID=17&topicID=58
Keep abreast of legal statutes affecting practice. For instance, knowledge or strong suspicion of child or elder abuse must be reported to DSS no matter how much you worry about the effect such a report may have on your relationship with your client. There is, however, no mandated reporting of spousal abuse. Duty-to-warn standards also supersede confidentiality. In cases where you are told of a plan to harm another individual, you may be required to break confidentiality in order to protect the intended victim.
Please
e-mail us any relevant links
that you find, so we may include them in future versions of this course.
Thank you!
It is advisable to consult with an attorney if you have questions or concerns about your obligation in your state.
Physical
violence in intimate relationships almost always is accompanied by psychological
abuse and, in one-third to over one-half of cases, by sexual abuse (59,
75, 131, 258, 272). For example, among 613 abused women in Japan, 57%
had suffered all three types of abuse—physical, psychological, and
sexual. Only 8% had experienced physical abuse alone (485). In Monterrey,
Mexico, 52% of physically abused women had also been sexually abused by
their partners (191). In Le'n, Nicaragua, among 188 women who were
physically abused by their partners, only 5 were not also abused sexually,
psychologically, or both (131).
Most women who suffer any physical aggression generally experience multiple
acts over time. In the Le'n study, for example, 60% of women abused
in the previous year were abused more than once, and 20% experienced severe
violence more than six times. Among women reporting any physical aggression,
70% reported severe abuse (130). The average number of physical assaults
in the previous year among currently abused women surveyed in London was
seven (308); in the US in 1997, three (436).
In surveys of partner violence, women usually are asked whether or not
they have experienced any of a list of specific actions, such as being
slapped, pushed, punched, beaten, or threatened with a weapon.
Asking behavioral questions—for example, “Has your partner
ever physically forced you to have sex against your will?”—yields
more accurate responses than asking women whether they have been “abused”
or “raped” (127). Surveys generally define
physical acts more severe than slapping, pushing, shoving, or throwing
objects as “severe violence.”
Measuring “acts” of violence
does not describe the atmosphere of terror that often permeates abusive
relationships. For example, in Canada's 1993 national violence survey
one-third of women who had been physically assaulted by a partner said
that they had feared for their lives at some point in the relationship
(378). Women often say that the psychological abuse and degradation are
even more difficult to bear than the physical abuse (57,
58, 96).
http://www.infoforhealth.org/pr/l11/l11chap2_1.shtml
|
On This Page Intimate partner violence—or IPV—is actual or threatened physical or sexual violence or psychological and emotional abuse directed toward a spouse, ex-spouse, current or former boyfriend or girlfriend, or current or former dating partner. Intimate partners may be heterosexual or of the same sex. Some of the common terms used to describe intimate partner violence are domestic abuse, spouse abuse, domestic violence, courtship violence, battering, marital rape, and date rape (Saltzman, et al. 1999). CDC uses the term intimate partner violence because it describes violence that occurs within all intimate relationships. Some of the other terms are overlapping and may be used to mean other forms of violence including abuse of elders, children, and siblings.
Back
to Top Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Costs of Intimate Partner Violence Against Women in the United States. Atlanta (GA): Centers for Disease Control and Prevention; 2003. Available on-line at http://www.cdc.gov/ncipc/pub-res/ipv_cost/ipv.htm. Coker AL, Smith PH, McKeown RE, Melissa KJ. Frequency and correlates of intimate partner violence by type: physical, sexual, and psychological battering. American Journal of Public Health 2000;90(4):553–9. Felitti V, Anda R, Nordenberg D, Williamson D, Spitz A, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine 1998;14(4):245–58. Gazmararian JA, Petersen R, Spitz AM, Goodwin MM, Saltzman LE, Marks JS. Violence and reproductive health; current knowledge and future research directions. Maternal and Child Health Journal 2000;4(2):79–84. Holtzworth-Monroe A, Bates L, Smutzler N, Sandin E. A brief review of the research on husband violence: part I: maritally violent versus nonviolent men. Aggression and Violent Behavior 1997;2(1):65–99. National Research Council. Understanding Violence Against Women. Washington (DC): National Academy Press; 1996. p. 74–80. Paulozzi LJ, Saltzman LA, Thompson MJ, Holmgreen P. Surveillance for homicide among intimate partners—United States, 1981–1998. CDC Surveillance Summaries 2001;50(SS-3):1–16. Roizen J. Issues in the epidemiology of alcohol and violence. In: Martin SE, editor. Alcohol and Interpersonal Violence: Fostering multidisciplinary perspectives. Bethesda (MD): National Institute on Alcohol Abuse and Alcoholism; 1993. p. 3–36. NIAAA Research Monograph No. 24. Saltzman LE, Fanslow JL, McMahon PM, Shelley GA. Intimate Partner Violence Surveillance: Uniform definitions and recommended data elements. Atlanta: National Center for Injury Prevention and Control; 1999. Straus MA, Gelles, RJ, editors. Physical Violence in American Families: Risk factors and adaptations to violence in 8,145 families. New Brunswick (NJ): Transaction Books; 1990. Tjaden P, Thoennes N. Full Report of the Prevalence, Incidence, and Consequences of Intimate Partner Violence Against Women: Findings from the National Violence Against Women Survey. Report for grant 93-IJ-CX-0012, funded by the National Institute of Justice and the Centers for Disease Control and Prevention. Washington (DC): NIJ; 2000. Tjaden P, Thoennes N. Extent, Nature, and Consequences of Intimate Partner Violence: Findings from the National Violence Against Women Survey. Report for grant 93-IJ-CX-0012, funded by the National Institute of Justice and the Centers for Disease Control. Washington (DC): NIJ; 2000. Wisner CL, Gilmer TP, Saltzman LE, Zink TM. Intimate partner violence against women: do victims cost health plans more? Journal of Family Practice 1999;48(6):439–43. |
AM I BEING ABUSED? Checklist Look over the following questions. Think about how you are being treated and how you treat your partner. Remember, when one person scares, hurts or continually puts down the other person, it’s abuse. Does your partner.... ____Embarrass or make fun of you in front of your friends or family? ____Put down your accomplishments or goals? ____Make you feel like you are unable to make decisions? ____Use intimidation or threats to gain compliance? ____Tell you that you are nothing without them? ____Treat you roughly - grab, push, pinch, shove or hit you? ____Call you several times a night or show up to make sure you are where you said you would be? ____Use drugs or alcohol as an excuse for saying hurtful things or abusing you? ____Blame you for how they feel or act? ____Pressure you sexually for things you aren’t ready for? ____Make you feel like there "is no way out" of the relationship? ____Prevent you from doing things you want - like spending time with your friends or family? ____Try to keep you from leaving after a fight or leave you somewhere after a fight to "teach you a lesson"? Do You... ____Sometimes feel scared of how your partner will act? ____Constantly make excuses to other people for your partner’s behavior? ____Believe that you can help your partner change if only you changed something about yourself? ____Try not to do anything that would cause conflict or make your partner angry? ____Feel like no matter what you do, your partner is never happy with you? ____Always do what your partner wants you to do instead of what you want? ____Stay with your partner because you are afraid of what your partner would do if you broke up? If any of these are happening in your relationship, talk to someone. Without some help, the abuse will continue. Your Domestic Violence Survival Kit Protecting Yourself in a Dangerous Relationship Print and Carry with you If you are still in the relationship: Think of a safe place to go if an argument occurs; avoid rooms with no exits (bathroom) or rooms with weapons (kitchen). Think about and make a list of safe people to call. Keep change with you at all times. Memorize all important numbers. Establish a code word or sign so that family, friends, teachers or coworkers know when to call for help. Think about what you will say to your partner if he or she becomes violent. Remember you have the right to live without fear and violence. Your Personal Safety Plan The following steps are my plan for increasing my safety and preparing to protect myself in case of further abuse. Although I can't control my abuser's violence, I do have a choice about how I respond and how I get to safety. I will decide for myself whether and when I will tell others that I have been abused or that I am still at risk. Friends, family and coworkers can help protect me, if they know what is happening and what they can do to help. To increase my safety, I can do some or all of the following: When I have to talk to my abuser in person, I can ________________________________ When I talk to my abuser on the phone, I can ___________________________________ I will have a code word for my family, coworkers or friends, so they know when to call for help for me. My code word is ________________ When I feel a fight coming on, I will try to move to a place that is lowest risk for getting hurt such as (at work)__________, (at home)____________, (in public)_________________. I can tell my family, coworkers, boss or a friend about my situation. I feel safe telling: ______________________________________________ I can use an answering machine or ask my coworkers, friends or other family members to screen my calls and visitors. I have the right to not receive harassing phone calls. I can ask to help screen my phone calls. (home)________ (work) _____________ I can keep change for phone calls with me at all times. I can call any of the following people for assistance or support if necessary and can ask them to call the police if they see my abuser bothering me. Friend _______________________________________ Relative ______________________________________ Coworker _____________________________________ Counselor _____________________________________ Shelter _______________________________________ Other ________________________________________ When leaving work I can: _________________________________________________ When walking, riding or driving home, if problems occur, I can: _____________________ I can attend a support group for women who have been abused. Support groups are:_______ ____________________________________________________________________ Telephone numbers I need to know: Police/Sheriff's Department: ___________________ Probation officer: _________________ Domestic violence/sexual assault program:________________ Counselor: ________________ Clergy: _____________________ Lawyer: ___________________ Other: ____________________ After you have left the relationship: Change your phone number. Screen calls. Save and document all contacts, messages, injuries or other incidents involving the batterer. Change locks if the batterer has a key. Avoid staying alone. Plan how to get away if confronted by an abusive partner. If you have to meet your partner, do it in a public place. Vary your routine. Notify school and work contacts. Call a shelter for battered women. The National Domestic Violence Hotline 1-800-799-SAFE
(7233) 1-800-787-3224 (TDD)
|
http://www.infoforhealth.org/pr/l11/l11chap3.shtml
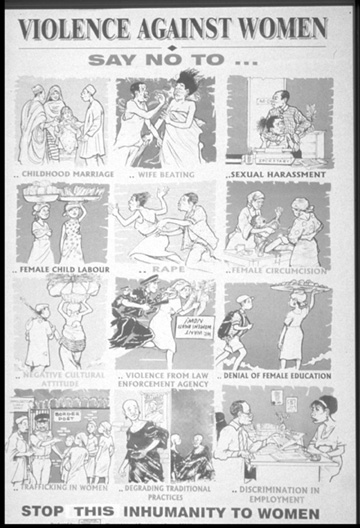
Women, Law and Development Centre Nigeria
As this poster from Nigeria illustrates, violence against women takes many forms. Often, social and cultural norms condone gender-based violence.
You may be becoming or already are a victim of abuse if you:
If you are abused:
Look out for men who:
http://www.womanabuseprevention.com/html/abuse_signs.html
Things You Can Do To Stay Safe
Are you a child or teenager living in a home where violence occurs, either
between your parents or your brothers and sisters?
If you answered yes, you should know that as a child living in an abusive
household there are things that you can do to be safe.
You should not get in the middle of a fight between your parents or brothers
and sisters, even if they ask you for help. This will not make the fighting
stop, and you may get hurt.
If you want to help the abused person ask how or simply dial 911, learn
important numbers including family and local emergency agencies, and go
over a safety or escape plan with the abused person.
Tips on calling 911:
When dialing 911 there are ways to make the response quicker, and to ensure
your safety. First tell the operator your name and address, tell them
what is going on and where this is happening, and you should tell them
if this has happened before.
Before an emergency situation occurs you should know:
*Your full name
*Your complete address including city, state and zip code
*Your entire phone number with area code
*What situations will lead you to call 911. If domestic violence is occurring
in your house, you might want to make up a code word with the abused parent
or sibling. If he/she uses that word then you will call 911
During an emergency situation you should know:
*Dialing 911 can reach police, the fire department or ambulance
*Try to remain calm
*When the 911 operator answers, state the problem briefly and give your
full name and address
*Do not hang up the phone until the operator says to
Asking For Help
Asking for help does not mean you are going to get in trouble, but if
you do get into trouble call the police again or speak to a trusted adult.
Trusted adults can include your teachers, ministers, coaches or family
members. If your parents are separated, divorced or never married, the
school should know who can and cannot pick you up from school. If the
person who is abusive visits your school or tries to remove you, please
notify a teacher or the principal. They can help you decide what to do
next.
If you need someone to talk to, there is help for you at school or somewhere
in your community.
Don't Blame Yourself
As a child living in an abusive home, it’s easy to blame yourself
and think that what is going on is your fault. You think "If I would
be quieter, better at school, neater, more respectful and so on and so
on." Living there, you must know that no matter how hard you try,
it does not stop. You are not the problem.
If the abused person or the abuser at some time needs to leave the home
for safety reasons, remember again this is not your fault. The abuser
in your home has a problem. This person chooses to be violent or controlling.
There is help for abusers. This help can come after you call the police
or through counseling. The abuser needs to learn that he/she does not
have the right to use violence, threats or intimidation to get what he/she
wants. Staying may seem dangerous or even stupid to you, but there are
reasons and some of them include your safety. Talk to the abused person,
talk to a teacher, or call a hotline and make a safety plan. For more
help, or someone to talk to please check the links section or call the
National Domestic Violence Hotline at 1-800-799-SAFE.
-------------
Department of Health and Human Services:
HELPING CHILDREN WHO WITNESS DOMESTIC
VIOLENCE
HHS Secretary Tommy G. Thompson today announced a new initiative
to help children who witness domestic violence to develop into healthy,
well-adjusted adults and prevent the cycle of violence from continuing
from one generation to the next.
The initiative, called "Safe and Bright Futures
for Children," will incorporate evidence-based
practices such as treatment for child and adolescent trauma, mentoring
and mental health services while also addressing risk and protective factors
to negate the cyclical effects of violence. It will encourage the
integration of these services at the local and regional level by building
collaborations of community, faith-based or other programs that identify,
assess, treat and provide long-term services.
"Each year, there are nearly 700,000 documented incidents of domestic
violence that threaten the well-being of children and families across
our nation," Secretary Thompson said. "This new effort will
provide preventive services and support to help children affected by this
violence to enjoy a safe and bright future and to break the cycle of violence.
We want to provide our youth with the skills and tools they need to make
healthy choices in their lives."
Research has found that activities that involve
and empower youth in their families, schools and communities can help
protect them from harm. Under the new effort, HHS expects to provide funding
for demonstration projects nationwide to serve children and adolescents
who witness or are exposed to domestic violence.
A significant percentage of children who
witness domestic violence eventually become abusers or victims of abuse.
In addition, children who witness domestic violence are more likely to
exhibit behavioral and physical health problems including depression,
anxiety and violence towards peers. Adolescents are also more likely to
attempt suicide, abuse drugs and alcohol, run away from home, engage in
teenage prostitution and commit sexual assault crimes.
U.S. Department of Health & Human Services • 200 Independence
Avenue, S.W. • Washington, D.C. 20201
http://www.hhs.gov/news/press/2003pres/20031008.html
Please go to the:
WORKSHOP
ON CHILDREN EXPOSED TO VIOLENCE:
CURRENT STATUS, GAPS, AND RESEARCH PRIORITIES
WORKSHOP SPONSORS:
National Institute of Child Health and Human Development (NICHD)
National Institute on Drug Abuse (NIDA)
National Institute of Mental Health (NIMH)
Fogarty International Center (FIC)
Office of Behavioral and Social Sciences Research (OBSSR)
Office of the Assistant Secretary for Planning and Evaluation (ASPE)
Centers for Disease Control and Prevention (CDC)
Substance Abuse and Mental Health Services Administration (SAMHSA)
Department of Health and Human Services (DHHS)
National Institute of Justice (NIJ)
Department of Justice
Office of Special Education Programs (OSEP)
Department of Education
|
This information packet provides an introduction to the dynamics, prevalence and consequences of teen dating violence. The packet explores issues specific to teen dating violence, examines current provision of support services for teens and presents information about a variety of promising prevention /intervention strategies. While some awareness materials such as booklets, checklists and posters are included, the intent of packet contents is to examine some of the key dating violence issues currently facing teens and their advocates. Material within the packet has been organized into categories according to current issues (see the Cover/Table of Contents). Following the Overview, a Key Issues section begins with a brief review of Teen Dating Violence Public Policy, followed by information about Health Concerns for Teen Dating Violence Survivors, Use of Violence by Girls and Boys in Heterosexual Teen Relationships, Service Provision Challenges and Changing Approaches in Prevention. The packet includes articles and referral information designed to promote increased knowledge on each key issue and concludes with a Fact Sheet, Statistics Sheet, Bibliography, and Resource Lists designed to help readers gain to access Prevention/Education, Intervention Programs and Direct Service Tools, Websites and Videos.
|
|
|||||||||||||||||||||||||
| SCREAMS IN A VACUUM Gay
male domestic violence and abuse
shares a great deal of similarities with its heterosexual
counterpart: frequency (approximately one in every four couples);
manifestations (emotional, physical, financial, sexual, etc);
co-existent situations (unemployment, substance abuse, low self-esteem);
victims' reactions (fear, feelings of helplessness, hyper vigilance);
and reasons for staying (love, can work it out, things will change,
denial) are some examples. But significant differences, unique
issues and deceptive myths are just as much part of the phenomenon.
Intra-lesbian Violence By: Lori Haskell Recently, the extent to which domestic violence is a gender issue has been the subject of debate, since violence takes place within lesbian relationships. Gender is socially constructed and, as such, is always present in human relationships. Gender is relevant to men's violence against women and to intra-lesbian battering, but gender plays out differently in the significantly different relational contexts. Because lesbian battering doesn't neatly fit into the theoretical model of heterosexual battering, it doesn't mean that we throw out our theory. A more productive approach would be to understand the continuities and discontinuities between violence in heterosexual and lesbian relationships. Obviously, there will be some similarities in why acts of physical violence are perpetrated in intimate relations, but there will be many differences as well between heterosexual and gay/lesbian relationships. The only way to develop a more complete and nuanced picture of the underlying dynamics is to contextualize our understanding; otherwise we may take the regressive step of proposing a purely psychological model which does not take social relations into account. Instead, we need to understand the forces of systemic subordination, such as heterosexism, sexism, racism, classism and differences in abilities, as these contribute to the shape violence in intimate relationships may take. Specifically, how are lesbian lives shaped, constrained and limited by the systems of oppression? To what degree and finally with what effect? We need to question whether the form and function of lesbian battering is the same as 'wife abuse' perpetrated by men against their female intimates. What both forms of abuse may share is the function of social control, albeit for entirely different reasons. Heterosexual men internalize the belief of male dominance, that is, that they are entitled to control their female partners in order to keep their privilege and dominance in place. Men's violence against women in intimate relationships is inextricably a part of male entitlement, a belief in men's right to control women and in male superiority. These beliefs are widely reinforced institutionally throughout our culture. Unlike heterosexual woman abuse, there are no wider cultural messages reinforcing lesbian superiority over their partners, or women's entitlement to exert control over their intimates to explain why some women may abuse their female partners. In a lesbian relationship, on the other hand, the sense of isolation, invisibility and silence that is often the result of homophobia and heterosexism increases the dependency of the partners on each other. This increased dependency and isolation may result in an increased need to control one's partner, especially in relationships where one lesbian passes as heterosexual while her partner does not, or when one partner seeks more independence or separation. These disruptions may pose a threat to the integrity of the relationship. This could result in a lesbian partner responding with emotional or physical violence as an attempt to control her partner and keep her in the relationship. Additionally, a consequence of internalized sexism and homophobia may very likely be decreased self-worth and possibly self hate. This sense of powerlessness and worthlessness that a lesbian may feel about herself can be transferred onto her partner. It is much easier to batter and violate someone you view with contempt, especially when that contempt is socially produced and reinforced through homophobia. Internalized homophobia and sexism are manifestations of oppression. Although these oppressions have clear psychological dimensions in terms of how they are manifested, they are still socially constructed, and gender is always implicated. This distinction between seeing a phenomenon as socially constructed versus one that is purely psychological is not just a matter of semantics. How we theorize and understand the problem gives direction to how we develop our strategies and interventions. If we see lesbian battering as a consequence of psychological problems, the approach would be to offer treatment to the individual, devoid of any attention to the social context of the relationship. If, however, we see the problem as socially constructed as a result of the intersections of different oppressions, then our approach is also one of social change, including creating safer communities, connection and support for lesbians, while working to eradicate homophobia and heterosexism. It is unlikely that physical violence, coercion and control characterize lesbian relationships to the same extent that repeated research has shown in random samples of women's experiences in heterosexual relationships. There is no historical and contemporary legacy legitimizing physical violence in lesbian relationships as there is underpinning men's violence against women in intimate relationships. Clearly this is a fundamental difference in the gender dynamics at play in violence in heterosexual and lesbian/gay relationships. We need a body of methodologically sound empirical research to document the pervasiveness, scale, effect and impact of violence in lesbian relationships. This would help reveal the differences and similarities between lesbian and heterosexual relationships. Lori
Haskell is a psychologist, researcher and educator on issues
of violence against women and children. |
| Contact: Gay Partner Abuse Project 416.876.1803 |
To read the course material, go now to: Lesbian, Gay, Bisexual and Trans (LGBT) Communities and Domestic Violence: Information and Resources by Mary Allen for the National Resource Center on Domestic Violence (NRCDV) (2007) Domestic violence in LGBT communities is about abuse of power, manipulation, exploitation, oppression and barriers to service. This collection has been designed for domestic violence program advocates, activists working in LGBT communities and those wishing to become allies.
|
Women
consistently cite similar reasons that they remain in abusive relationships:
fear of retribution, lack of other means of economic support, concern
for the children, emotional dependence, lack of support from family and
friends, and an abiding hope that “he will change” (10, 131,
330, 413, 488). In developing countries women cite the unacceptability
of being single or unmarried as an additional barrier that keeps them
in destructive marriages (169, 368, 488).
At the same time, denial and fear of social stigma often prevent women
from reaching out for help. In surveys, for example, from 22% to almost
70% of abused women say that they have never told anyone about their abuse
before being asked in the interview (see Table 3). Those who reach out
do so primarily to family members and friends. Few have ever contacted
the police.
http://www.infoforhealth.org/pr/l11/l11chap2_3.shtml
A wide range of studies agrees on several factors at each of these levels that increase the likelihood that a man will abuse his partner:
Questionnaire:
ARE YOU BEING ABUSIVE?
Below are a series of questions that may assist you in understanding if your behavior is abusive or violent. Domestic violence includes not only the more visible physical manifestations but also includes verbal, emotional and sexual forms of behavior. If you answer yes to any of these questions you may wish to seek assistance through the Gay Partner Abuse Project or another source of professional assistance. Recognizing your behavior is the first step towards making change.
http://www.gaypartnerabuseproject.org/html/abusive.html
| PHASE
1. TENSION BUILDING |
PHASE
2. ACUTE BATTERING |
PHASE
3. KINDNESS AND LOVING BEHAVIOR |
| Victim compliant, good behavior. Batterer
experiences increased tension. |
Batterer
unpredictable, claims loss of control. |
Batterer
often apologetic, attentive. Victim has mixed feelings. Batterer is manipulative. Victim feels guilty and responsible. Batterer promises change. Victim considers reconciliation *court: often the victim must appear in court during this time |
|
Note:In
an effort to disrupt the idea that only men perpetrate abuse,
the pronouns used on this web site and in our literature that
refer to perpetrators are predominantly female. Feel free to imagine
the information using varied gender pronouns, such as he, ze or
s/he. |
|
|
|||||||||||||||||
| |
ABUSE IS NOT S/M AND S/M IS NOT ABUSE
Whether you are topping, or bottoming, or both, these are some questions to ask yourself:
|
||||||||||||||||
|
Copyright
© 2003 Northwest Network.All Rights Reserved. |
|||||||||||||||||
"Many cultures hold that men have the right to control their wives' behavior and that women who challenge that right—even by asking for household money or by expressing the needs of the children—may be punished. In countries as different as Bangladesh, Cambodia, India, Mexico, Nigeria, Pakistan, Papua New Guinea, Tanzania, and Zimbabwe, studies find that violence is frequently viewed as physical chastisement—the husband's right to “correct” an erring wife (10, 39, 94, 189, 204, 233, 303, 341, 407, 488). As one husband said in a focus-group discussion in Tamil Nadu, India, “If it is a great mistake, then the husband is justified in beating his wife. Why not? A cow will not be obedient without beatings” (233)." (Ending violence against women, a report from the Center for Communications Programs, Johns Hopkins University at http://www.infoforhealth.org/pr/l11/l11chap2_2.shtml#top)
From the University of Michigan Health System Tools & Resources: Culture and Domestic Violence
Help Minority Battered Women Seek Assistance!
Cultural Barriers for African American Victims of Domestic Violence
Internal Barriers:
External Barriers:
Sources:
Campbell, DW. "Nursing Care of African-American Battered Women: Afrocentric
Perspectives." AWHONN's Clinical Issues in Nursing. 4(3): 407-415.
1993.
Robinson, MS. "Battered Women: An African American Perspective."
The ABNF Journal. pp. 81-84. 1991.
Cultural Barriers for Asian Victims of Domestic Violence
Internal Barriers:
External Barriers:
Source:
Asian Task Force Against Domestic Violence
Cultural Barriers for Latino Victims of Domestic Violence
Internal Barriers:
External
Barriers:
Source: "Bauer
HM, et.al. "Barriers to health care for abused Latina and Asian Immigrant
Women." Journal of Health Care for the Poor and Underserved. Vol
(1) 11. pp. 33-44. 2000.
AYUDA Family Violence and Prevention Fund
Culture and Domestic Violence: A Select Bibliography
Adams, DL. (Ed.) Health Issues for Women of Color: A Cultural Diversity Perspective. Thousand Oaks, CA: Sage Publications, 1995.
Berenson AB, Stiglich NJ, et al. "Drug Abuse and other Risk Factors for Physical Abuse in Pregnancy among White non-Hispanic, Black, and Hispanic Women." American Journal of Obstetrics and Gynecology. 164: pp. 1491-1499. 1991.
Burns, MC (ed) The Speaking Profits US: Violence in the Lives of Women of Color. Seattle, WA: Center for the Prevention of Sexual and Domestic Violence.1986.
Campbell JC, Campbell DW. "Cultural Competence in the Care of Abused Women." Journal of Nurse Midwifery. 41(6): pp. 457-462.1996.
Campbell, DW. "Nursing Care of African-American Battered Women: Afrocentric Perspectives." AWHONN's Clinical Issues. 4 (3): pp. 407-415. 1993.
Denis RE, Key LJ, et al. "Addressing Domestic Violence in the African American Community." Journal of Health Care for the Poor and Underserved. 6(2): pp. 284-293.1995.
Galanti, GA. Caring for Patients of Different Cultures. Philadelphia, PA: University of Pennsylvania Press, 1991.
Huisman, KA. "Wife Battering in Asian American Communities: Identifying the Service Needs of an Overlooked Segment of the US Population." Violence Against Women. 2(3) pp. 260-283. 1996.
Panigua, F. Assessing and Treating Culturally Diverse Clients. Thousand Oaks, CA: Sage Publications Inc. 1994.
Richie, BE. Understanding Family Violence Within US Refugee Communities: A Training Manual. Washington, DC: Refugee Women In Development, Inc, 1988.
Thompson MP, Kaslow NJ. "Partner Violence, Social Support, and Distress Among Inner-City African American Women." American Journal of Community Psychology. 28(1) pp. 127-143. 2000.
Sorenson SB. "Violence Against Women: Examining ethnic differences and commonalties." Evaluation Review. 20(3) p. 123. 1996.
Volpp L, Main L. Working with Battered Immigrant Women: A Handbook to Make Services Accessible. San Francisco, CA: Family Violence Prevention Fund, 1995.
White, EC. Chain Chain Change: For Black Women in Abusive Relationships. Seattle. WA: Seal Press. 1994.
http://www.med.umich.edu/multicultural/ccp/cdv.htm
Despite the obstacles, many women eventually do leave violent
partners—even if after many years, once the children are grown (129,
227). In Le'n, Nicaragua, for example, the likelihood that an abused
woman will eventually leave her abuser is 70%. The median time that women
spend in a violent relationship is five years. Younger women are more
likely to leave sooner (131).
Studies suggest a consistent set of factors that propel women
to leave an abusive relationship: The
violence gets more severe and triggers a realization that “he”
is not going to change, or the violence begins to take a toll on the children.
Women also cite emotional and logistical support from family or friends
as pivotal in their decisions to leave (52, 62, 65, 69,
202, 413).
Leaving an abusive relationship is a process. The process often
includes periods of denial, self-blame, and endurance before women come
to recognize the abuse as a pattern and to identify with other women in
the same situation. This is the beginning of disengagement and recovery.
Most women leave and return several times before they finally leave once
and for all (264).
Regrettably, leaving does not necessarily
guarantee a woman's safety. Violence sometimes continues and may even
escalate after a woman leaves her partner (227). In fact, a woman's risk
of being murdered is greatest immediately after separation (60).http://www.infoforhealth.org/pr/l11/l11chap2_3.shtml
Since Congress enacted the Violence Against Women Act as part of the Violent Crime Control and Law Enforcement Act of 1994, HHS has significantly expanded its efforts. HHS quadrupled resources for battered women's programs and shelters, created a national toll-free domestic violence hotline (1-800-799-SAFE), and expanded efforts to raise awareness of domestic violence in the workplace and among health care providers. In fiscal year 2001, Congress appropriated $244.5 million for HHS programs to prevent violence against women, including $2.2 million for the National Domestic Violence Hotline. President Bush's fiscal year 2002 budget increases that commitment to $251 million.
BACKGROUND
The landmark Violence Against Women Act (VAWA), administered by HHS and the Department of Justice (DOJ), provided funding to hire more prosecutors and improve domestic violence training among prosecutors, police officers, and health and social services professionals. It also provided for more shelters, counseling services and research into causes of violence and effective community campaigns to reduce violence against women.
The VAWA set new federal penalties for those who cross state lines to continue abuse of a spouse or partner, making interstate domestic abuse and harassment a federal offense. It also requires states to honor protective orders issued in other states and gives victims the right to mandatory restitution and the right to address the court at the time of sentencing.
In 1995, HHS and DOJ created the National Advisory Council on Violence Against Women, consisting of experts from law enforcement, media, business, sports, health and social services, and victim advocacy. The council works with both the public and private sectors to promote greater awareness about the problem of violence against women and its victims, to help devise solutions, and to advise the federal government on these issues. In October 2000, the council released an "Agenda for the Nation on Violence Against Women," which outlines recommendations for future efforts to build on the early successes of the VAWA.
In October 2000, Congress reauthorized the Violence Against Women Act programs as part of the Victims of Trafficking and Violence Protection Act of 2000.
HHS PROGRAMS UNDER VAWA
Grants for battered women's shelters. The VAWA significantly expanded HHS funding for battered women's shelters. Since the law was passed, HHS' grants for these programs more than quadrupled from $27.6 million in fiscal year 1994 to $116.9 million in fiscal year 2001. The reauthorization legislation enacted in 2000 increased the minimum grant amount for each state from $400,000 to $600,000. These resources also support related services, such as community outreach and prevention, children's counseling, and linkage to child protection services.
The National Domestic Violence Hotline. In 1996, HHS launched the National Domestic Violence Hotline, a 24-hour, toll-free service that provides crisis assistance and local shelter referrals for callers across the country. Since then, the hotline has responded to more than 500,000 calls, mostly from individuals who have never before reached out for assistance. HHS funds the hotline through a grant to the Texas Council on Family Violence. The hotline number is 1-800-799-SAFE, and the TDD line for the hearing impaired is 1-800-787-3224.
Grants to reduce sexual assault. HHS provides grants to states for rape prevention and education programs conducted by rape crisis centers or similar nongovernmental, nonprofit entities. The funds support educational seminars, the operation of hotlines, training programs and other activities to increase awareness of and help prevent sexual assault, including programs targeted to students. HHS funding for the program in fiscal year 2001 is $44.1 million. In addition, $7 million from the Preventive Health and Health Services Block Grant is earmarked for rape prevention programs.
Coordinated community responses. The Centers for Disease Control and Prevention (CDC) works to build new community programs aimed at preventing intimate partner violence and strengthening existing community intervention and prevention programs. The CDC is currently funding a total of 10 projects and received $5.9 million to fund these efforts in fiscal year 2001. CDC has also conducted the National Violence Against Women survey and completed a study on the cost of violence against women. CDC funds numerous cooperative agreements with state health departments to improve understanding of the issue.
Outreach to runaway, homeless youth. HHS funds a program to provide street-based outreach and education, including treatment, counseling and provision of information and referrals to runaways, homeless and street youth who have been subjected to or are at risk of sexual abuse. The program was appropriated at $15 million for fiscal year 2001.
OTHER HHS INITIATIVES
National resource centers. The Administration for Children and Families (ACF) funds a network of five national resource centers that provide information, technical assistance and research findings related to domestic violence. The network includes the National Resource Center on Domestic Violence (800-537-2238), the Battered Women's Justice Project (800-903-0111), the Resource Center on Child Custody and Protection (800-527-3223), the Health Resource Center on Domestic Violence (888-792-2873), and the Sacred Circle Center on Violence Against Native Women (605-341-2050). The CDC funds the National Electronic Violence Against Women Resource Network (VAWnet) and the National Sexual Assault Resource Center (http://www.nsvrc.org). The VAWnet is an online resource for advocates working to end domestic violence, sexual assault and other violence in the lives of women and their children. The electronic library is available at http://www.VAWnet.org.
Child welfare grants. HHS has funded 26 grants over three years to local programs to stimulate collaboration between child welfare agencies and domestic violence providers. These projects train child welfare staff to identify and respond appropriately to instances of domestic violence in their caseloads. In addition, HHS has awarded 13 training stipends to schools of social work to develop curricula and train social workers in family violence.
Welfare Reform and Family Violence. In 1996, Congress enacted the Personal Responsibility and Work Opportunities Reconciliation Act, which included provisions to help welfare recipients who are victims of domestic violence move successfully into work. Specifically, the provisions give states the option to screen welfare recipients for domestic abuse; refer them to counseling and supportive services; and temporarily waive any program requirements that would prevent recipients from escaping violence or would unfairly penalize them.
Guidelines on effective intervention. Supported by HHS and DOJ funding, the National Council of Juvenile and Family Court Judges developed a best practice guidelines for handling child protection cases involving domestic violence. The group published "Effective Intervention in Domestic Violence and Child Maltreatment Cases: Guidelines for Policy and Practice" in 1999. In 2000, following a competitive process, six sites were selected to demonstrate the effectiveness of community collaborations in implementing the report's recommendations.
Mental health, substance abuse and violence. The Substance Abuse and Mental Health Services Administration (SAMHSA) supports several programs addressing substance abuse and mental health issues among victims of violence. These efforts include a five-year study designed to develop effective integrated service programs for women and their children affected by violence and co-occurring mental and addictive disorders. The program has yielded several comprehensive curricula to train substance abuse, mental health and other health and human services professionals on working with women victims of violence. Another multi-year SAMHSA grant program focuses on the connection among domestic violence, mental illness, substance abuse and homelessness among women and their children by assessing the effectiveness of time-limited intensive treatment, housing, support and family preservation services to homeless mothers and their dependent children.
Research initiatives. In 2000, the Agency for Healthcare Research and Quality (AHRQ) awarded $5.5 million to fund four comparative studies examining the effectiveness of intervention programs offered in health care settings. AHRQ and the nonprofit Family Violence Prevention Fund also jointly sponsor a Scholar in Residence, who is developing better ways to assess health system interventions. In addition, the National Institute of Mental Health (NIMH) funds a number of research studies focusing on the mental health consequences of violence, treatments for the traumatic consequences of violence, and factors that influence the initiation of physically aggressive behavior in intimate relationships. These studies have significant implications for preventing and reducing the mental health consequences of domestic violence.
Related programs. HHS agencies run and support a wide range of programs that provide services, information and other resources to address violence against women as part of broader program goals. For example, the Administration on Aging (AoA) funds elder abuse prevention programs in all 50 states that focus on the prevention of elder abuse, neglect and exploitation - including domestic violence. In addition, many HHS programs aim to strengthen families, prevent the abuse of women and children, and help families provide a healthy and safe environment for children. These programs include the Promoting Safe and Stable Families program and Child Abuse Prevention and Treatment Act grants.
Where
can I get help if I am being abused?
The National Domestic Violence Hotline, available 24 hours a day, 7 days
a week, provides services in English and Spanish. If you or someone you
know is being abused, contact the Hotline at (800) 799-7233. The Rape,
Abuse and Incest National Network also operates a 24-hour, 7-day-a-week
hotline for victims of sexual assault. The Network automatically connects
callers to a rape crisis center in their community where they can find
counseling and support. You can reach the Network at (800) 656-4673.
Back to top
Intimate Partner Violence
Like
all violence, intimate partner violence perpetration is a learned behavior
that can be changed or prevented.
Safety Tips for You and Your Family
If
you are the victim of intimate partner violence, do not blame yourself.
Talk with people you trust and seek services. Contact your local battered
women’s shelter or the National Domestic Violence Hotline at
800-799-SAFE (7233), 800-787-3224 TDD, or www.ndvh.org/.
They can provide you with helpful information and advice.
If
you are or think you may become a perpetrator of intimate partner
violence contact the National Domestic Violence Hotline at 800-799-SAFE
(7233), 800-787-3224 (TDD), or www.ndvh.org/.
They can provide you with helpful contact information.
Recognize
early warning signs for physical violence such as a partner's extreme
jealousy, controlling behavior, verbal threats, history of violent
tendencies or abusing others, and verbal or emotional abuse.
Know
what services are available for victims and perpetrators of intimate
partner violence and their children in case you or a friend should
need help.
Learn more about intimate partner violence. Information is available in libraries, from local and national domestic violence organizations, and through the Internet. The more you know about intimate partner violence, the easier it will be to recognize it and help friends who may be victims or perpetrators.
In Your Community
Support increased access to services for victims and perpetrators of intimate partner violence as well as for their children.
Coordinate community initiatives to strengthen safety networks for women who experience violence.
Increase public awareness to help decrease and prevent intimate partner violence.
CDC Resources
Preventing
intimate partner violence requires the support and contribution of a variety
of partners.
National Sexual Violence Resource Center
www.nsvrc.org
877-739-3895
A clearinghouse of information, resources, and research, related to all
aspects of sexual violence. Activities include collecting, reviewing,
cataloging, and disseminating information related to sexual violence;
coordinating efforts with other organizations and projects; providing
technical assistance and customized information packets on specific topics;
and maintaining a website with current information including upcoming
conferences, funding opportunities, job announcements, research, special
events, links to state and territory coalitions, and other resources.
The NSVRC also produces a biannual newsletter, The Resource; recommends
speakers for conferences; coordinates national sexual assault awareness
activities; and identifies emerging policy issues and research needs.
The NSVRC serves coalitions, local rape crisis centers, government and
tribal entities, colleges and universities, service providers, researchers,
allied organizations, policy-makers, and the general public.
National Violence Against Women Prevention Research Center
www.vawprevention.org
843-792-2945
Helps prevent violence against women by advancing knowledge about prevention
research and fostering collaboration among advocates, practitioners, policy
makers, and researchers. Over the next five years, the NVAWPRC and its
partners at CDC will be involved in a number of activities to accomplish
this mission. The NVAWPRC serves as a clearinghouse for prevention strategies
and keeps researchers and practitioners aware of training opportunities,
policy decisions, and recent research findings. The NVAWPRC website also
offers the latest research on violence against women as a resource to
everyone involved in the field of violence prevention so they can better
do their work.
Violence Against Women Electronic Network (VAWnet)
www.vawnet.org
Provides support for the development, implementation, and maintenance
of effective violence against women intervention and prevention efforts
at the national, state, and local levels through electronic communication
and information dissemination. VAWnet participants, including state domestic
violence and sexual assault coalitions, allied organizations, and individuals,
have access to online database resources. Network members are able to
engage in information sharing, problem-solving, and issue analysis via
electronic mail and a series of issue-specific forums facilitated by nationally
recognized experts in the field of violence against women. VAWnet also
operates an extensive searchable electronic library available to the general
public, providing links to external sources; an “In the News”
section; and access to articles and audio and video resources focused
on intimate partner and sexual violence and related issues.
Other Resources
The
materials presented herein are for information purposes only. We have
not screened each individual or organization that appears on this site
or that is electronically linked to this site. The appearance of an individual
or organization on this site is not intended as an endorsement. We urge
all users of this site to conduct their own investigations of the products
or services identified herein.
This list is not comprehensive but presents some of the major national
violence against women resources and national organizations addressing
violence against women.
If you are experiencing an emergency, call 911 or your local emergency
number immediately.
American Bar Association
Commission on Domestic Violence
phone: 202.662.1737/1744
fax: 202.662.1594
www.abanet.org/domviol/home.html
The members of the Commission help resolve problems in family law, criminal
law, victims' and individuals' rights, judicial administration, tort and
civil rights litigation, and immigration law. Representatives of other
professional organizations serve on the Commission to help develop a national
domestic violence agenda as well as to enhance existing policies and solutions
in the constantly changing fields of state and federal domestic violence
law.
American College of Obstetricians and Gynecologists (ACOG)
409 12th Street SW
Washington, DC 20024-2188
phone: 202.638.5577
www.acog.org
ACOG is the nation's leading group of professional providing health care
for women. ACOG is dedicated to the advancement of women's health through
education, advocacy, practice, and research.
American Institute on Domestic Violence
2116 Rover Drive
Lake Havasu City, AZ 86403
phone: 928.453.9015
fax: 775.522.9120
www.aidv-usa.com
The American Institute on Domestic Violence offers on-site workshops and
conference presentations addressing the corporate cost of domestic violence
in the workplace.
Asian and Pacific Islander Institute on Domestic Violence
942 Market Street, 2nd Floor
San Francisco, CA 94102
phone: 425.954.9964
fax: 415.954.9999
www.apiafh.org/
The Asian and Pacific Islander Institute on Domestic Violence is a national
network that works to raise awareness in Asian & Pacific Islander
communities about domestic violence; expand leadership and expertise within
Asian & Pacific Islander communities about prevention, intervention,
advocacy and research; and promote culturally relevant programming, research,
and advocacy by identifying promising practices.
Battered Women's Justice Project
phone: 800-903-0111
fax: 218-722-0779
http://www.bwjp.org/
The Battered Women’s Justice Project consists of three sections,
criminal justice, civil justice and the defense of battered women charged
with crimes.
Communities Against Violence Network
www.cavnet2.org
Communities Against Violence Network (CAVNET) provides an interactive
online database of information; an international network of professionals;
and real-time voice conferencing with professionals and survivors, from
all over the world, using the Internet. CAVNET seeks to address violence
against women, youth violence, and crimes against people with disabilities
Corporate Alliance to End Partner Violence
2416 E. Washington Street, Suite E Bloomington, IL 61704-4472
phone: 309.664.0667
fax: 309.664.0747
www.caepv.org
The Corporate Alliance to End Partner Violence (CAEPV) is a national non-profit
alliance of corporations and businesses throughout the U.S. and Canada,
united to educate and aid in the prevention of partner violence. CAEPV
provides technical assistance and materials to help corporations and businesses
address domestic violence in their workplaces.
The Family Violence Prevention Fund
383 Rhode Island Street, Suite 304
San Francisco, CA 94103-5133
phone: 415.252.8900
fax: 415.252.8991
www.endabuse.org
The Family Violence Prevention Fund is a national non-profit organization
most noted for it’s national public education campaign “There’s
No Excuse for Domestic Violence.” The Fund also has a National Health
Initiative on Domestic Violence that works to train health care providers
throughout the nation to recognize signs of abuse and to intervene effectively
to help battered women. Hallmarks of this initiative include: the Ten-State
Pilot Health Care Response to Domestic Violence program working to develop
and implement state wide plans for a comprehensive health care system
response to domestic violence; and the FVPF's Health Resource Center on
Domestic Violence, which acts as the nation's clearinghouse for information
on the health care response to domestic violence. Other projects include
the Judicial Education Project, the Child Welfare Project, the National
Workplace Resource Center on Domestic Violence, and the Battered Immigrant
Women's Rights Project. Their Health Resource Center on Domestic Violence
Provides resource and training material, technical assistance, information
and referrals, and models for local, state and national health policymakers
to support those interested in developing a comprehensive health care
response.
The Institute on Domestic Violence in the African American Community
University of Minnesota/School of Social Work
290 Peters Hall
1404 Gortner Ave.
St. Paul, MN 55108-6142
phone: 877.643.8222
fax: 612.624.9201
www.dvinstitute.org
The Institute on Domestic Violence in the African American Community seeks
to create a community of African American scholars and practitioners working
in the area of violence in the African American community, further scholarship
in the area of African American violence, raise community consciousness
of the impact of violence in the African American community, inform public
policy, organize and facilitate local and national conferences and training
forums, and to identify community needs and recommend best practices.
Minnesota Center Against Violence and Abuse
School of Social Work, University of Minnesota 105 Peters Hall, 1404 Gortner
Avenue St. Paul, Minnesota 55108-6142
phone: 612.624.0721
fax: 612.625.4288
www.mincava.umn.edu
The Minnesota Center Against Violence and Abuse (MINCAVA) is an electronic
clearinghouse located in the School of Social Work of the University
of Minnesota with educational resources about all types of violence,
including higher education syllabi, published research, funding sources,
upcoming training events, individuals or organizations which serve as
resources, and searchable databases with over 700 training manuals, videos
and other education resources. MINCAVA is also part of a is a cooperative
project - the Violence Against Women Online Resources - between the Center
and the United States Department of Justice, Office of Justice Programs,
Violence Against Women Office. This website
provides law, criminal justice, and social service professionals with
current information on interventions to stop violence against women.
National Coalition Against Domestic Violence
P.O. Box 18749 Denver, CO 80218 phone: 303.839.1852 fax: 303.831.9251
www.ncadv.org
The National Coalition Against Domestic Violence (NCADV) is a membership
organization of domestic violence coalitions and service programs. NCADV
provides training, technical assistance, legislative and policy advocacy,
promotional and educational materials and products on domestic violence;
coordinates a national collaborative effort to assist battered women in
removing the physical scars of abuse; and works to raise awareness about
domestic violence.
National Domestic Violence Hotline
PO Box 161810
Austin, TX 78716
phone hotline: 1.800.779.SAFE (7233)
tty:1.800.787.3224
administrative: 512.453.8117
fax: 512.453.8541
www.ndvh.org
The National Domestic Violence Hotline connects individuals to help in
their area using a nationwide database that includes detailed information
on domestic violence shelters, other emergency shelters, legal advocacy
and assistance programs, and social service programs. Help is available
in English or Spanish, 24 hours a day, seven days each week. Interpreters
are available to translate an additional 139 languages.
National Latino Alliance for the Elimination of Domestic Violence
P.O. Box 322086 Ft. Washington Station New York, NY 10032
phone: 646-672-1404 or 1-800-342-9908 fax: 1-800-216-2404
www.DVAlianza.org
The National Latino Alliance for the Elimination of Domestic Violence
(the Alianza) is a group of nationally recognized Latina and Latino advocates,
community activists, practitioners, researchers, and survivors of domestic
violence working together to promote understanding, sustain dialogue,
and generate solutions to move toward the elimination of domestic violence
affecting Latino communities, with an understanding of the sacredness
of all relations and communities. Support from ACF/DHHS has allowed the
Alianza to establish El Centro: National Latino Research Center on Domestic
Violence and the Alianza Training and Technical Assistance (T/TA) Division.
National Network on Behalf of Battered Immigrant Women
http://www.endabuse.org/programs/immigrant/
The National Network on Behalf of Battered Immigrant Women was co-founded
in 1994 by the Family Violence Prevention Fund, AYUDA, NOW Legal Defense
and Education Fund and the National Immigration Project of the National
Lawyers Guild to nationally coordinate advocacy efforts aimed at removing
the barriers battered immigrant and children face when they attempt to
leave abusive relationships. Each organization provides leadership in
their area of expertise.
National Network to End Domestic Violence
660 Pennsylvania Ave. SE, Suite 303
Washington, DC 20003
phone: 202.543.5566
www.nnedv.org
The National Network to End Domestic Violence (NNEDV) is a membership
and advocacy organization of state domestic violence coalitions. NNEDV
provides legislative and policy advocacy on behalf of the state domestic
violence coalitions and, through the National Network to End Domestic
Violence Fund, provides training, technical assistance and funds to domestic
violence advocates.
National Resource Center on Domestic Violence
6400 Flank Drive, Suite 1300
Harrisburg, PA 17112-2778
phone: 800-537-2238
tty: 800-553-2508
fax: 717-545-9456
www.vawnet.org
The National Resource Center on Domestic Violence (NRC) provides comprehensive
information and resources, policy development and technical assistance
designed to enhance community response to and prevention of domestic violence.
There are 40 NRC publications, as well as NRC project descriptions and
project publication lists available via VAWnet. These NRC projects include
the Building Comprehensive Solutions to Domestic Violence Initiative,
the Public Education Technical Assistance Project, and VAWnet.
National Training Center on Domestic and Sexual Violence
2300 Pasadena Drive
Austin, TX 78757
phone: 512.407.9020
fax: 512.407.9022
www.ntcdsv.org
The National Training Center on Domestic and Sexual Violence develops
and provides innovative training and consultation, influences policy and
promotes collaboration and diversity in working to end domestic and sexual
violence. NTCDV has a staff of nationally known trainers and sponsor national
and regional conferences.
Rape, Abuse & Incest National Network (RAINN)
www.rainn.org
hotline: 800.656.HOPE
RAINN is the country’s only national rape hotline. RAINN works as
a call-routing system. When an individual calls RAINN a computer reads
the area code and first three digits of their phone number and routes
the call to the nearest member rape crisis center.
Sacred Circle: Native Resource Center to End Violence Against Native Women
PO Box 638
Kyle, SD 57752
phone: 877.733.7623 (red-road)
fax: 605.341.2472
www.sacred-circle.com
Provides technical assistance, policy development, training institutes,
and resource information regarding domestic violence and sexual assault
to develop coordinated agency responses in American Indian/ Alaska Native
tribal communities.
The Stalking Resource Center
c/o National Center for Victims of Crime
2000 M Street NW, Suite 480
Washington, DC 20036
phone: 202.467.8700 fax: 202.467.8701
www.ncvc.org
The Stalking Resource Center is a project of the National Center for Victims
of Crime, funded through the Violence Against Women Office, U.S. Department
of Justice. The Stalking Resource Center has established a clearinghouse
of information and resources to inform and support local, multi disciplinary
stalking response programs nationwide; developed a national peer-to-peer
exchange program to provide targeted, on-site problem-solving assistance
to VAWO Arrest grantee jurisdictions; and organized a nationwide network
of local practitioners representing VAWO grantee jurisdictions to support
their multi disciplinary approaches to stalking.
Federal Agencies
Department of Health and Human Services
Centers for Disease Control and Prevention
National Center for Injury Prevention and Control
Division of Violence Prevention
4770 Buford Highway, NE MS K-60
Atlanta, GA 30341
Fax: 770-488-4349
www.cdc.gov/injury
The National Center for Injury Prevention and Control (NCIPC) guides national
efforts to reduce the incidence, severity, and adverse outcomes of intentional
and unintentional injuries in the United States. As the lead federal agency
for injury prevention, NCIPC works closely with other federal agencies
and national, state, and local organizations to reduce injury, disability,
and premature death. NCIPC’s priority areas for violence prevention
are: child maltreatment, intimate partner violence, sexual violence, suicide
and youth violence. Project and activities focus on primary prevention
of violence through a public health approach.
Department of Health and Human Services,
The Office on Women’s Health,
National Women’s Health Information Center (NWHIC)
Office on Women's Health
Department of Health and Human Services
200 Independence Avenue, SW
Room 730B Washington, DC 20201
Phone: 202-690-7650
Fax: 202-205-2631
www.4woman.gov/
The National Women's Health Information Center (NWHIC) is the Office on
Women's Health's clearinghouse for women's health information. The NWHIC
provides a gateway to the vast array of Federal and other women's health
information resources. This site provides links to a wide variety of women's
health-related material developed by the Department of Health and Human
Services, other Federal agencies, and private sector resources.
U.
S. Department of Justice, Office for Victims of Crime
Office for Victims of Crime Resource Center
National Criminal Justice Reference Service
P.O. Box 6000
Rockville, MD 20849––6000
1–800–627–6872
(TTY 1–877–712-9279)
www.ojp.usdoj.gov/ovc/
The Office for Victims of Crime (OVC) was established by the 1984 Victims
of Crime Act (VOCA) to oversee diverse programs that benefit victims of
crime. OVC provides substantial funding to state victim assistance and
compensation programs——the lifeline services that help victims
to heal. The agency supports trainings designed to educate criminal justice
and allied professionals regarding the rights and needs of crime victims.
OVC also sponsors an annual event in April to commemorate National Crime
Victims Rights Week (NCVRW).
U.S. Department of Justice
Violence Against Women Office
810 7th Street, NW
Washington, DC 20531
Phone (202) 307-6026
Fax (202) 307-3911
TTY (202) 307-2277
www.ojp.usdoj.gov
The Violence Against Women Office works with victim advocates and law
enforcement in developing grant programs that support a wide range of
services for victims of domestic violence, sexual assault, and stalking,
including: advocacy, emergency shelter, law enforcement protection, and
legal aid. Additionally the Violence Against Women Office is leading efforts
nationally and abroad to intervene in and prosecute crimes of trafficking
in women and children and is addressing domestic violence issues in international
fora.
Trauma
is the German word for "nightmare," but in English, it is used for any
kind of injury, physical or psychological. As a survivor of abusive relationships,
you have suffered trauma which probably seems like a "nightmare."
Stress is a force that changes the shape of things (including people).
This traumatic relationship has changed you—you will never be the
same again. You are recovering from a great deal of stress on your body
and mind as a result of this trauma.
Because of this stressful, traumatic relationship you may exhibit the
signs of post-traumatic stress. It will take time and hard work to completely
heal.
http://www.nwnetwork.org/articles/5.html
Please go to the
based upon
the SAMHSA Substance Abuse Treatment
and Domestic Violence, Treatment Improvement Protocol (TIP) Series, Number
25.
Excerpted here:
:
If a client believes that she is in immediate danger from a batterer,
the treatment
provider should respond to this situation before addressing any other
issues. If
necessary, they should suspend the screening interview for this purpose,
and assist
the client in developing a safety plan (Appendix B). The provider should
refer the
client to a domestic violence program, and allow the client to use the
telephone to
contact identified resources, if appropriate (Appendix C).
: The provider can identify and ask about several
indicators of abuse. The most
obvious indicators are physical injuries, especially patterns of untreated
injuries to
the face, neck, throat, and breasts. Other indicators may include a history
of
relapse or noncompliance with substance abuse treatment plans; inconsistent
explanations for injuries and evasive answers when questioned about them;
complications in pregnancy (including miscarriage, premature birth, and
infant illness or birth defects); stress-related
illnesses and conditions (such as headache, backache, chronic pain, gastrointestinal
distress, sleep disorders, eating disorders, and fatigue); anxiety-related
conditions
(such as heart palpitations, hyperventilation, and panic attacks); sad,
depressed
affect; or talk of suicide. In addition, the client may mention being
afraid of the
partner or his "anger" problem or controlling behaviors. Agency
medical protocols
may need to be reviewed in order to respond most appropriately to survivors.
: Always interview clients about domestic violence
in private, and do not reveal any
information about disclosure of domestic violence to other family members.
• : Ask about violence using concrete examples and hypothetical
situations rather
than vague, conceptual questions.
: In framing screening questions, it is extremely
important to convey to the survivor
that there is no justification for the battering and that substance abuse
is no
excuse. Questions such as, "Does he blame his violence on
his alcohol or drug use?"
or, "Does he use alcohol (or other drugs) as an excuse for his violence?"
serve the
dual purpose of determining whether the client's partner may be a substance
abuser while reinforcing to her that substance abuse is not the real reason
for his
violence.
: Addictions counselors should be trained to screen clients for domestic
violence, to
assist in safety planning and to provide information about resources.
The
counselors should also know when domestic violence experts should be contacted.
Violence assessment requires in-depth knowledge and skill and should be
conducted
by a domestic violence expert.
• : Providers should be aware that the overlap
between child abuse and domestic
violence is 60-70%, thus they should be alert to the possibility that
the mother of a
child who has been or is being abused by her partner is also being abused
herself,
and vice versa.
• : The provider should refer the client to or encourage the client
to use other
resources, such as medical care, if injured, police or the criminal justice
system,
shelters or other victim programs.
: Once the client has entered substance abuse treatment,
a treatment plan that
includes a safety plan (see Appendix B) should be developed. In addition,
the
provider should support the client in avoiding contact with the perpetrator,
if the client goal is to avoid contact. A subsequent relapse prevention
plan should address domestic violence issues, including safety planning
and avoiding contact with the perpetrator, if appropriate.
: Survivors appear to benefit by participating in
same-sex treatment groups that do
not use confrontational techniques. Providers
should keep in mind that victims of
domestic violence have been systematically deprived of their self-determination
as
part of the abuse. Thus, program models that emphasize powerlessness as
a
treatment strategy should be aware that this might be counter to recovery
needs
related to domestic violence. When external limits are necessary,
they should also
take into account that she may be placing her safety above success in
the
treatment program.
• Staff training in the areas of crisis intervention
and co-occurring mental health
problems such as PTSD is important so that treatment providers can respond
effectively. Referrals should also be made whenever appropriate
for specialized
counseling.
Part 11: Screening, Referral, and Treatment of Batterer Clients
A discussion of family relationships is an element
of all substance abuse screening
interviews. This component of the interview should be used to address
the issue of
domestic violence and controlling behaviors with male clients.
. To initially gauge the possibility that a client
is being abusive toward his family
members, the interviewer can ask whether he/she thinks violence and controlling
behaviors against a partner is justified in some situations, using
a third person
example.
•Ask specific, concrete questions (e.g.,
"What happens when you lose your
temper?"). Be direct and candid; avoid
euphemisms such as, "Is your relationship
with your partner troubled?" Instead, talk
about "his violence and controlling
behaviors" and keep the focus on "his behavior." Ask about
specific violent and
controlling behaviors (e.g., "When you hit her, was it a slap
or a punch?", "Do you
take her car keys away?", "Damage her property?", "Threaten
to hurt or kill
her?").
• In asking screening questions, substance abuse treatment
providers must be
careful not to enable a batterer to place the blame for the battering
on the victim
or the drug.
•Become familiar with batterers' rationalizations
for their behavior, and with ways
to counter them. Examples are:
• Minimizing "I only pushed her,"
"She bruises easily," "She exaggerates." To
counter
minimizing, say, "Any violence is unacceptable and harmful to the
victim."
• Citing good intentions "She
gets hysterical so I have to slap her to calm her down.
To counter a claim of good intentions, say, "Any violence is unacceptable
and
harmful to the victim. You are the only person responsible for your violent
behavior."
• Blaming the use of alcohol and drugs "I'm
not myself when I drink." To counter a
blaming use of alcohol and drugs, say, "Any
violence is unacceptable and harmful
to the victim. You are the only person responsible for your violent behavior;
abuse/use of alcohol and drugs does not make it okay."
• Claiming loss of control: "Something
snapped," "I can only take so much," "I was
so angry, I didn't know what I was doing." To counter claiming loss
of control, say
"Any violence is unacceptable and harmful to the victim. Being angry
or 'out of control'
does not make it okay."
• Blaming the partner "She drove
me to it," "She really knows how to get to me." To
counter blaming the victim, say, "Any violence is unacceptable and
harmful to the
victim. You are the only person responsible for your violent behavior;
her behavior
does not make your violent acts okay."
• Blaming someone or something else: "I
was raised that way," "My probation
officer is putting a lot of pressure on me," "I've been out
of work." To counter a
blaming someone else, say, "Any violence is unacceptable and harmful
to the victim.
You are the only person responsible for your violent behavior. Being out
of work is
no excuse for being violent."
: Perpetrators' often attempt to maintain contact
with their partner in order to
control her time or access to support. When establishing rules,
providers should be
careful to assure that contact with the victim is for a legitimate reason,
and does
not give the perpetrator an opportunity for on-going control or violence.
• : Once there is an indication that a client has assaulted or been
controlling of a
partner, the provider should contact a domestic violence expert, either
for
consultation or referral.
• : Treatment providers should try to ensure
the safety of those who have been or
may become victims of the client, in particular his partner and children,
during any
crisis during treatment, including to be aware of the providers duty to
warn.
Appendix D.
• : Treatment providers, in some cases, may
require that batterers sign a "no
contact contract" or a "no offensive contact contract."
(Appendix E). that states
that the client will refrain from using violence and controlling behaviors
both inside
and outside the program. If the provider requires signing contracts, they
should
have in place a way to verify whether or not the batterer has complied
with the
contract, and have specific consequences if they have not.
• : Domestic violence staff sometimes interviews the batterer's
partner in order to
obtain salient information about his dangerousness to himself, his partner,
and
others. This type of collateral interviewing is quite different from that
practiced in
the substance abuse treatment setting and should only be performed by
someone with specialized skills and expertise in domestic violence.
Any information obtained in that interview should never to revealed to
the
perpetrator, without the explicit request by the victim. If the victim
does request that
information be shared with the perpetrator, the provider must address
safety
concerns with the victim.
The relationship between substance abuse and violent and controlling behavior
should
be addressed in relapse prevention planning. The following information
may be useful in
developing the plan:
• Exactly when in relation to substance abuse do the violence and
controlling
behaviors occurs
• How much of the violent behavior occurs while the batterer is
drinking or on other
drugs.
• What substances are used before the violent act.
• What feelings and thoughts precede and accompany the use of alcohol
or other
drugs or precede the violence or controlling behaviors.
• Whether alcohol or other drugs are used to "recover"
from the violent incident.
After identifying the chain of events that precede
or trigger violent episodes, provider
and client should together formulate strategies for modifying those behaviors
and
recognizing emotions and thoughts that contribute to violent and controlling
behavior.
Providers should be alert to signs that batterer clients are misinterpreting
the 12-Step philosophy to justify or excuse continued violence and controlling
behaviors.
Another danger is that they will call their victims "codependent"
in order to shift
blame for the battering onto the woman.
Referrals to batterers intervention programs should be a routine part
of the
treatment, and referrals to family or couples counseling
should only be made after the
client has completed a batterers' intervention program and has remained
nonviolent
for a specified period of time.
If a provider is asked or subpoenaed to testify in a custody or visitation
hearing on
behalf of the batterer, it is standard practice for the information provided
to be
limited to information contained in the file, such as treatment status
and progress in
treatment. Providers should refrain from offering opinions relating to
the client's
potential future threat for violence or controlling behavior and his parental
fitness.
Part III: Specific Recommendations for Family-Based Treatment
: Family-based treatment or couples counseling is
generally contraindicated in
situations where one partner is violent or controlling toward the other.
In part this
is because asking or expecting the victim to disclose battering in front
of the
perpetrator may further endanger her. Such programs should only be utilized
after
the perpetrator has completed a batterers' intervention program and has
remained nonviolent and non-controlling for a specified period of time.
Providers
should have defined criteria and a method to determine whether the victim
safety
is assured before recommending family-based treatment or couples counseling.
: If the victim (whether the victim is the client or the spouse or mother
of the
perpetrator's children) has separated or is attempting to separate from
the
perpetrator, the provider should not attempt to facilitate or encourage
reconciliation or reunification with the perpetrator. These attempts are
inappropriate and are likely to endanger the victim.
: If the victim is choosing to stay with the perpetrator, any family work
must assure
that the victim is safe and must protect her confidentiality. The provider
must be
willing to give her information that will increase her safety. This may
mean getting
the perpetrator (if he is the client) to sign a release of information.
Until safety can
be assured, it may mean working separately with the perpetrator and with
the
victim.
• : Treatment providers should support other family members in taking
steps to be
safe, including restricted visitation by children, limited contact with
the
victim/partner, or other steps.
• : Discussions of co-dependency in cases of battering are inappropriate,
because it
too easily can be used to blame the victim for the violence.
• : See Appendix F, Domestic Abuse Project, Training and Research
UPDATE, "Why
Couples Counseling May be Inappropriate for Violent Relationships."
Part IV:Legal Issues
There are many Federal, State, and local regulations
that bear upon domestic
violence, particularly ORS Family Abuse Prevention Act and Mandatory Arrest
law, and
the 1994 Violence Against Women Act (VAWA). Providers
need to
be aware of such issues as restraining orders, duty to warn, the legal
obligation to
report threats and past crimes, and confidentiality.
: Substance abuse treatment providers should be familiar with relevant
Federal,
State, and local regulations as well as with the legal resources available
to victims
of domestic abuse. (Appendix C)
: Providers should have information available to victims ONLY about restraining
orders and how to get them, mandatory arrest laws, law enforcement and
district
attorney services available, including child support enforcement, victim
advocates
and Crime Victim Compensation programs.
• : Providers should provide identified batterers with information
about the criminal
nature of domestic violence, and possible negative consequences to criminal
justice
system involvement, as part of a message that domestic violence is not
acceptable behavior (as opposed to suggestions for how to "beat the
system.")
Part V: Establishing Linkages
This Protocol recommends linkages between substance abuse treatment programs
and domestic violence programs and among other agencies as well.
• : Treatment providers and domestic violence support workers should
foster a new
way of thinking about linkages on the systems level. Both fields would
benefit from
a coordinated system that could addresses the multiple supportive interventions
needed by victims who are abusing substances and multiple means to stop
perpetrators who are abusing substances from continuing to be violent.
: In the absence of systemic reform, substance abuse treatment providers,
domestic
violence experts, and legal or other relevant professionals should plan
treatment
collaboratively.
: Initial meetings between organizations trying to establish linkages
should include
discussion of the origins of both communities in order to help each understand
the
other's beliefs and attitudes.
• : Linkages should address needs for housing, child care, emotional
and physical
safety, health and mental health care, economic stability, legal
protection, vocational and educational services, parenting training, and
support and
peer counseling, among others.
• : A legal professional or legal service is the best resource for
resolving problems
that pertain to individual clients' involvement in the civil and criminal
justice
systems. Providers should be aware of the resources available and have
established relationships, as appropriate.
: Substance abuse treatment providers should assess their ability to screen
for
violence and create a safety plan, as well as their knowledge of legal
issues related
to domestic violence, and develop a plan to assure staff competency.
• : Providers should work collaboratively with domestic violence
specific programs to
assure adequate staff training. Cross-training for both disciplines is
important, and
providers should participate in training domestic violence programs on
alcohol and
drug treatment abuse.
• : Providers should participate, as appropriate, in a coordinated
community response
to domestic violence.
Appendix
E—No Offensive Contact Contract
MULTNOMAH COUNTY OREGON
DEPARTMENT OF ADULT COMMUNITY JUSTICE
DOMESTIC VIOLENCE UNIT
407 NE 12TH AVE. PORTLAND, OR 97232
(503) 248-5056
FAX (503) 306-5517
Review date: ______________________
Offender's name/SID # (please print): ______________________________________
THIS DOCUMENT REFERS TO: ___________________________________
(Name of victim partner/designated party) Please print
DEFINITION OF OFFENSIVE CONTACT
Domestic Violence is a pattern of behaviors in which one partner attempts
to establish or
maintain power and control over the other through physical, sexual, and/or
psychological
abuse. There are many ways you may control a person through threat and
intimidation without
actually using physical violence, particularly if you have used physical
violence against that
person in the past. As a result of your violence against your partner,
you are directed to refrain
from behaviors that constitute domestic violence. These behaviors are
called offensive contact.
Offensive contact is defined as engaging in physical,
sexual or psychological abuse of another
person.
Physical abuse
Physical abuse is defined as any forceful or violent action directed at
someone
else.
Some examples of physical abuse are: Slapping, choking or strangling,
maiming, stabbing,
punching, scratching, wrestling, kicking, spanking, grabbing, pinching,
biting, burning,
pushing, poking, restraining, pulling hair, picking a person up, carrying
them, throwing them
bodily, forcing them to eat or drink something, stopping them from getting
medical attention,
stealing or hiding their medication, throwing things at or near a person,
using any object or
weapon against them, physically making a person do something against their
will (i.e.: forcing
them to sit down, hang up the phone, get into the car, put something down,
stay at home, etc.).
These are only some examples of physical abuse. There are many other types
of physical abuse
that are not listed here, but they are stir/ offensive contact.
Please initial here if you understand what is meant by physical abuse.
Sexual Abuse
Sexual abuse is defined as any non-consenting (not freely agreed to) sexual
act or
behavior.
Some examples of sexual abuse are: Forcing or demanding sexual activity
when a person says no, when
they are asleep, when they are drunk or high, when a person is afraid
of being hurt (or that the
children will be hurt or sexually abused) if they say no, when you have
not asked first, asking for or
demanding sexual activity after you have physically or psychologically
abused a person (for example
hitting, pushing or threatening them).
Physically attacking the sexual parts of a persons" body, pulling
or ripping their clothes off, demanding
or forcing a person to engage in sexual behaviors that they do not like
or that embarrasses, humiliates,
scares or hurts them.
These are only some examples of sexual abuse. There are many more types
of sexual abuse that are
not listed here, but they are still offensive contact.
________ Please initial here if you understand what is meant by sexual
abuse.
Psychological Abuse
Psychological abuse is defined as behaviors (words or actions) that are
used to
intimidate, create fear, or threaten another person, and can be determined
to be a
pattern of harassment.
Some examples of psychological abuse are:
*Acting like you are going to physically or sexually abuse them or the
children.
*Holding your hand up like you are going to slap, hit or punch, throw
things, making them
think that you are going to throw or punch something, hurt the children,
use a weapon o r
break something, etc.
*Using your physical size to intimidate a person (standing over them,
backing them against a
wall, blocking them from leaving a room or the house), getting in a person's
face, using a
commanding/intimidating tone of voice, yelling at them, the children or
pets, etc.
*Using threatening behaviors like: driving recklessly with a person (and/or
the children) in
the car, throwing things, hurting a pet, punching walls, threatening a
person with an object
or weapon, slamming doors, smashing or breaking things, following a person
around to watch
what they are doing, pulling the phone out of the wall, etc.
*Specifically doing things you were told not to do by a person (including
contacting them at
work, calling them late at night, etc).
*Stalking a person by driving or walking past their residence, place of
work or their friends
and family members residences or places of work. Or having a person known
to the victim drive
or walk past the residences, places of work, etc.
*Telling him/her you are going to physically or sexually abuse him/her.
*Saying that if they do something you are going to slap, smack, shoot,
stab, hit, etc. them, the
children or the pet(s), making vague threats (i.e.: "You're going
to get it" or "You better not
piss me off" or "Now you're in trouble", etc), or referring
to abuse you have subjected them or
someone else to in the past like, "Do you want me to have to hit
you again," or "You're acting like
you did the last time I hit you," or " When you do that you
remind me of my ex-partner and you
know what happened to them."
*Making threats to do things to a person (and/or the children), such as
saying you will take
away the children (or have them taken away), that you will have them arrested,
will not pay
child support, have an affair, hurt a pet, commit suicide, start drinking
or using drugs
(especially when you have been violent to them while under the influence),
etc.
*White psychological abuse may not cause immediate physical damage, it
is very powerful
because you have hurt a person (and/or the children) in the past. All
threats and threatening
behaviors are abusive because you have shown that you may back up your
threats with violence.
These are only some examples of psychological abuse. There are many more
types of
psychological abuse that are not listed here, but they are still offensive
contact.
_______Please initial here if you understand what is meant by psychological
abuse.
If authorized to have non-offensive contact with
the victim in my case(s), I agree to abide by
the definition of offensive contact listed herein. I further understand
that any violation of this
definition may result in my arrest, and revocation of the contact directive
established.
Offender's signature:________________________________________
Parole/Probation Officer's name (please print):________________________________
Parole/Probation Officer's
signature:_________________________________________
Original: File
Copies: Offender
Victim/partner/designated party
Document created by Lane County Parole and Probation, Eugene, OR. Used
and modified by Muitnomah County with permission.
Revised 8/05/99 (Microsoft Word: Hafowler: Offensive contact)
Batterer
intervention programs (BIPs) are designed for men arrested for domestic
violence and for men who would be arrested if their actions were public.
These programs usually consist of educational classes or treatment
groups, but may include other intervention elements such as extensive
evaluation, individual counseling, or case management. Because 80% of
batterers are referred by the criminal justice system, one set of implicit
goals for BIPs includes justice and accountability (Healey, Smith &
O'Sullivan, 1998 ), goals that have not been adequately recognized in
evaluations of BIPs. Another goal of BIPs is victim safety. Most standards
for BIPs specify that service providers consider victim safety implications
when implementing interventions such as contacting victims for information
about the batterer ( Austin & Dankwort, 1997 ; 1999 ). A final goal
for BIPs is rehabilitation and behavioral changes such as skill building,
attitude change, and emotional development.
The details of conducting batterer intervention programs are readily available
(e.g. Edleson & Tolman, 1992 ; Pence & Paymar, 1993 ; Russell
& Frohberg, 1995 ; Sonkin & Durphy, 1997 ; Stordeur & Stille,
1989 ). The purpose of this paper is to look not at what batterer programs
do, but rather at the effectiveness of these programs. Knowledge about
batterer program effectiveness is important for several reasons. Increasingly,
courts are referring men convicted of domestic abuse to batterers intervention
programs, suggesting a certain level of public confidence in the effectiveness
of these programs. Is that confidence justified? Second, victims of domestic
violence often want to remain in a relationship with their partner, and
are looking for help in changing his violent and controlling behavior.
Since a batterer seeking counseling is one of the strongest predictors
that a woman will return to her batterer ( Gondolf, 1988 ), advocates
are justifiably concerned that batterer programs not hold out a promise
of hope which may become a vehicle for injury. Third, people who work
with batterers are interested in outcomes so they can improve the level
of program effectiveness; for these people, the concern is less whether
batterer programs work, but how they work, for whom do they work best,
and which elements of the program are most important.
Controversies and Recent Studies of Batterer Intervention Program
Effectiveness by Larry Bennett, Ph.D and Oliver Williams, Ph.D. http://new.vawnet.org/category/Main_Doc.php?docid=373
Posttraumatic Stress Disorder, or PTSD, is a psychiatric disorder that can occur following the experience or witnessing of life-threatening events such as military combat, natural disasters, terrorist incidents, serious accidents, or violent personal assaults like rape. People who suffer from PTSD often relive the experience through nightmares and flashbacks, have difficulty sleeping, and feel detached or estranged, and these symptoms can be severe enough and last long enough to significantly impair the person's daily life.
PTSD is marked by clear biological changes as well as psychological symptoms. PTSD is complicated by the fact that it frequently occurs in conjunction with related disorders such as depression, substance abuse, problems of memory and cognition, and other problems of physical and mental health. The disorder is also associated with impairment of the person's ability to function in social or family life, including occupational instability, marital problems and divorces, family discord, and difficulties in parenting.
PTSD is not a new disorder. There are written accounts of similar symptoms that go back to ancient times, and there is clear documentation in the historical medical literature starting with the Civil War, when a PTSD-like disorder was known as "Da Costa's Syndrome." There are particularly good descriptions of posttraumatic stress symptoms in the medical literature on combat veterans of World War II and on Holocaust survivors.
Careful research and documentation of PTSD began in earnest after the Vietnam War. The National Vietnam Veterans Readjustment Study estimated in 1988 that the prevalence of PTSD in that group was 15.2% at that time and that 30% had experienced the disorder at some point since returning from Vietnam.
PTSD has subsequently been observed in all veteran populations that have been studied, including World War II, Korean conflict, and Persian Gulf populations, and in United Nations peacekeeping forces deployed to other war zones around the world. There are remarkably similar findings of PTSD in military veterans in other countries. For example, Australian Vietnam veterans experience many of the same symptoms that American Vietnam veterans experience.
PTSD is not only a problem for veterans, however. Although there are unique cultural- and gender-based aspects of the disorder, it occurs in men and women, adults and children, Western and non-Western cultural groups, and all socioeconomic strata. A national study of American civilians conducted in 1995 estimated that the lifetime prevalence of PTSD was 5% in men and 10% in women.
Most people who are exposed to a traumatic, stressful event experience some of the symptoms of PTSD in the days and weeks following exposure. Available data suggest that about 8% of men and 20% of women go on to develop PTSD, and roughly 30% of these individuals develop a chronic form that persists throughout their lifetimes.
The course of chronic PTSD usually involves periods of symptom increase followed by remission or decrease, although some individuals may experience symptoms that are unremitting and severe. Some older veterans, who report a lifetime of only mild symptoms, experience significant increases in symptoms following retirement, severe medical illness in themselves or their spouses, or reminders of their military service (such as reunions or media broadcasts of the anniversaries of war events).
In recent years, a great deal of research has been aimed at developing and testing reliable assessment tools. It is generally thought that the best way to diagnose PTSD-or any psychiatric disorder, for that matter-is to combine findings from structured interviews and questionnaires with physiological assessments. A multi-method approach especially helps address concerns that some patients might be either denying or exaggerating their symptoms.
An estimated 7.8 percent of Americans will experience PTSD at some point in their lives, with women (10.4%) twice as likely as men (5%) to develop PTSD. About 3.6 percent of U.S. adults aged 18 to 54 (5.2 million people) have PTSD during the course of a given year. This represents a small portion of those who have experienced at least one traumatic event; 60.7% of men and 51.2% of women reported at least one traumatic event. The traumatic events most often associated with PTSD for men are rape, combat exposure, childhood neglect, and childhood physical abuse. The most traumatic events for women are rape, sexual molestation, physical attack, being threatened with a weapon, and childhood physical abuse.
About 30 percent of the men and women who have spent time in war zones experience PTSD. An additional 20 to 25 percent have had partial PTSD at some point in their lives. More than half of all male Vietnam veterans and almost half of all female Vietnam veterans have experienced "clinically serious stress reaction symptoms." PTSD has also been detected among veterans of the Gulf War, with some estimates running as high as 8 percent.
1. Those who experience greater stressor magnitude and intensity, unpredictability, uncontrollability, sexual (as opposed to nonsexual) victimization, real or perceived responsibility, and betrayal
2. Those with prior vulnerability factors such as genetics, early age of onset and longer-lasting childhood trauma, lack of functional social support, and concurrent stressful life events
3. Those who report greater perceived threat or danger, suffering, upset, terror, and horror or fear
4. Those with a social environment that produces shame, guilt, stigmatization, or self-hatred
PTSD is associated with a number of distinctive neurobiological and physiological changes. PTSD may be associated with stable neurobiological alterations in both the central and autonomic nervous systems, such as altered brainwave activity, decreased volume of the hippocampus, and abnormal activation of the amygdala. Both the hippocampus and the amygdala are involved in the processing and integration of memory. The amygdala has also been found to be involved in coordinating the body's fear response.
Psychophysiological alterations associated with PTSD include hyper-arousal of the sympathetic nervous system, increased sensitivity of the startle reflex, and sleep abnormalities.
People with PTSD tend to have abnormal levels of key hormones involved in the body's response to stress. Thyroid function also seems to be enhanced in people with PTSD. Some studies have shown that cortisol levels in those with PTSD are lower than normal and epinephrine and norepinephrine levels are higher than normal. People with PTSD also continue to produce higher than normal levels of natural opiates after the trauma has passed. An important finding is that the neurohormonal changes seen in PTSD are distinct from, and actually opposite to, those seen in major depression. The distinctive profile associated with PTSD is also seen in individuals who have both PTSD and depression.
PTSD is associated with the increased likelihood of co-occurring psychiatric disorders. In a large-scale study, 88 percent of men and 79 percent of women with PTSD met criteria for another psychiatric disorder. The co-occurring disorders most prevalent for men with PTSD were alcohol abuse or dependence (51.9 percent), major depressive episodes (47.9 percent), conduct disorders (43.3 percent), and drug abuse and dependence (34.5 percent). The disorders most frequently comorbid with PTSD among women were major depressive disorders (48.5 percent), simple phobias (29 percent), social phobias (28.4 percent), and alcohol abuse/dependence (27.9 percent).
PTSD also significantly impacts psychosocial functioning, independent of comorbid conditions. For instance, Vietnam veterans with PTSD were found to have profound and pervasive problems in their daily lives. These included problems in family and other interpersonal relationships, problems with employment, and involvement with the criminal justice system.
Headaches, gastrointestinal complaints, immune system problems, dizziness, chest pain, and discomfort in other parts of the body are common in people with PTSD. Often, medical doctors treat the symptoms without being aware that they stem from PTSD.
PTSD is treated by a variety of forms of psychotherapy and drug therapy. There is no definitive treatment, and no cure, but some treatments appear to be quite promising, especially cognitive-behavioral therapy, group therapy, and exposure therapy. Exposure therapy involves having the patient repeatedly relive the frightening experience under controlled conditions to help him or her work through the trauma. Studies have also shown that medications help ease associated symptoms of depression and anxiety and help with sleep. The most widely used drug treatments for PTSD are the selective serotonin reuptake inhibitors, such as Prozac and Zoloft. At present, cognitive-behavioral therapy appears to be somewhat more effective than drug therapy. However, it would be premature to conclude that drug therapy is less effective overall since drug trials for PTSD are at a very early stage. Drug therapy appears to be highly effective for some individuals and is helpful for many more. In addition, the recent findings on the biological changes associated with PTSD have spurred new research into drugs that target these biological changes, which may lead to much increased efficacy.
This fact sheet describes elements common to many treatment modalities for PTSD, including education, exposure, exploration of feelings and beliefs, and coping-skills training. Additionally, the most common treatment modalities are discussed, including cognitive-behavioral therapy, pharmacotherapy, EMDR, group treatment, and psychodynamic treatment.
Treatment for PTSD typically begins with a detailed evaluation and the development of a treatment plan that meets the unique needs of the survivor. Generally, PTSD-specific treatment is begun only after the survivor has been safely removed from a crisis situation. If a survivor is still being exposed to trauma (such as ongoing domestic or community violence, abuse, or homelessness), is severely depressed or suicidal, is experiencing extreme panic or disorganized thinking, or is in need of drug or alcohol detoxification, it is important to address these crisis problems as a part of the first phase of treatment.
Cognitive-behavioral therapy (CBT) involves working with cognitions to change emotions, thoughts, and behaviors. Exposure therapy is one form of CBT that is unique to trauma treatment. It uses careful, repeated, detailed imagining of the trauma (exposure) in a safe, controlled context to help the survivor face and gain control of the fear and distress that was overwhelming during the trauma. In some cases, trauma memories or reminders can be confronted all at once ("flooding"). For other individuals or traumas, it is preferable to work up to the most severe trauma gradually by using relaxation techniques and by starting with less upsetting life stresses or by taking the trauma one piece at a time ("desensitization").
Along with exposure, CBT for trauma includes:
learning skills for coping with anxiety (such as breathing retraining or biofeedback) and negative thoughts ("cognitive restructuring"),
managing anger,
preparing for stress reactions ("stress inoculation"),
handling future trauma symptoms,
addressing urges to use alcohol or drugs when trauma symptoms occur ("relapse prevention"), and
communicating and relating effectively with people (social skills or marital therapy).
Pharmacotherapy (medication) can reduce the anxiety, depression, and insomnia often experienced with PTSD, and in some cases, it may help relieve the distress and emotional numbness caused by trauma memories. Several kinds of antidepressant drugs have contributed to patient improvement in most (but not all) clinical trials, and some other classes of drugs have shown promise. At this time, no particular drug has emerged as a definitive treatment for PTSD. However, medication is clearly useful for symptom relief, which makes it possible for survivors to participate in psychotherapy.
Eye Movement Desensitization and Reprocessing (EMDR) is a relatively new treatment for traumatic memories that involves elements of exposure therapy and cognitive-behavioral therapy combined with techniques (eye movements, hand taps, sounds) that create an alternation of attention back and forth across the person's midline. While the theory and research are still evolving for this form of treatment, there is some evidence that the therapeutic element unique to EMDR, attentional alternation, may facilitate the accessing and processing of traumatic material.
Group treatment is often an ideal therapeutic setting because trauma survivors are able to share traumatic material within the safety, cohesion, and empathy provided by other survivors. As group members achieve greater understanding and resolution of their trauma, they often feel more confident and able to trust. As they discuss and share how they cope with trauma-related shame, guilt, rage, fear, doubt, and self-condemnation, they prepare themselves to focus on the present rather than the past. Telling one's story (the "trauma narrative") and directly facing the grief, anxiety, and guilt related to trauma enables many survivors to cope with their symptoms, memories, and other aspects of their lives.
Brief psychodynamic psychotherapy focuses on the emotional conflicts caused by the traumatic event, particularly as they relate to early life experiences. Through the retelling of the traumatic event to a calm, empathic, compassionate, and nonjudgmental therapist, the survivor achieves a greater sense of self-esteem, develops effective ways of thinking and coping, and learns to deal more successfully with intense emotions. The therapist helps the survivor identify current life situations that set off traumatic memories and worsen PTSD symptoms.
Psychiatric disorders that commonly co-occur with PTSD include depression, alcohol/substance abuse, panic disorder, and other anxiety disorders. Although crises that threaten the safety of the survivor or others must be addressed first, the best treatment results are achieved when both PTSD and the other disorder(s) are treated together rather than one after the other. This is especially true for PTSD and alcohol/substance abuse.
Complex PTSD (sometimes called "Disorder of Extreme Stress") is found among individuals who have been exposed to prolonged traumatic circumstances, especially during childhood, such as childhood sexual abuse. Developmental research is revealing that many brain and hormonal changes may occur as a result of early, prolonged trauma, and these changes contribute to difficulties with memory, learning, and regulating impulses and emotions. Combined with a disruptive, abusive home environment that does not foster healthy interaction, these brain and hormonal changes may contribute to severe behavioral difficulties (such as impulsivity, aggression, sexual acting out, eating disorders, alcohol/drug abuse, and self-destructive actions), emotional regulation difficulties (such as intense rage, depression, or panic), and mental difficulties (such as extremely scattered thoughts, dissociation, and amnesia). As adults, these individuals often are diagnosed with depressive disorders, personality disorders, or dissociative disorders. Treatment often takes much longer than with regular PTSD, may progress at a much slower rate, and requires a sensitive and structured treatment program delivered by a trauma specialist.
There
is increasing consensus, as reflected in this declaration, that abuse
of women and girls, regardless of where and how it occurs, is best understood
within a “gender” framework because it stems in part from
women's and girls' subordinate status in society.
Article 2 of the UN Declaration clarifies that the definition of violence
against women should encompass, but not be limited to, acts of physical,
sexual, and psychological violence in the family and the community. These
acts include spousal battering, sexual abuse of female children, dowry-related
violence, rape including marital rape, and traditional practices harmful
to women, such as female genital mutilation (FGM). They also include nonspousal
violence, sexual harassment and intimidation at work and in school, trafficking
in women, forced prostitution, and violence perpetrated or condoned by
the state, such as rape in war.
http://www.infoforhealth.org/pr/l11/l11chap1_1.shtml#top
Legal Issues for South Asian Women
Please make sure that your patients know how to clear the history on their computers when they use the Internet for seeking assistance.
A caution on the use of Internet resources
http://www.gaypartnerabuseproject.org/html/history.html
CLEARING YOUR COMPUTER'S HISTORY
Windows keeps a chronological history on all web pages that are visited. It may be prudent for your safety to delete the record that you have visited this web page. If you choose to do so, it is a simple process (as described below) which will not in any way affect your computer other than to erase the fact that you have visited this and, depending on the version of Windows that you are running, other web pages.
Clearing your computer's history of a web page you visited (most Windows versions):
1. Click the tab marked History in the toolbar of Internet Explorer.
2. Your web pages visited history will appear on the left.
3. Under today's pages, highlight each Gay Partner Abuse Project's page name showing (should be last entries) and hit the delete key on your keyboard on each page name highlighted.
4. Exit your Internet browser. This method will only delete the selected pages.
If you have an older Windows version you will have to follow these steps instead:
1. On your Internet browser click on Tools
2. Click Internet Options
3. In the section called Temporary Internet Files, click Delete Files then click OK
4. In the section called History, click Delete History then click OK
NOTE: This method will delete all pages visited since history began.
By doing this you will not harm your computer in any way. However, should your partner click on History, he may realize that you or someone has deleted the history records. If this happens, and you are the only other person using that computer, a good reason to give for your actions (if necessary) would be that you heard or read that by deleting these temporary history files your computer would be faster and waste less disk space, which is true.
 Domestic
Violence Hotline Numbers by State
Domestic
Violence Hotline Numbers by StateContinue
to Part II of the course ![]()

Partner & Spousal Abuse
To
take the post-test, please return to
http://www.psychceu.com/materialsandtests/login.asp
888-777-3773
|
|

All material included in this course is either in the public domain, or used with express permission. |
We do adhere to the American Psychological Association's Ethical Principles of Psychologists. Our courses are carefully screened by the Planning Committee to adhere to APA standards. We also require authors who compose Internet courses specifically for us follow APA ethical standards. Many of our courses contain case material, and may use the methods of qualitative research and analysis, in-depth interviews and ethnographic studies. The psychotherapeutic techniques depicted may include play therapy, sandplay therapy, dream analysis, drawing analysis, client and therapist self-report, etc. The materials presented may be considered non-traditional and may be controversial, and may not have widespread endorsement within the profession. www.psychceu.com maintains responsibility for the program and its content. |