|
|
This course meets the qualifications for 3 hours of continuing education
Introduction
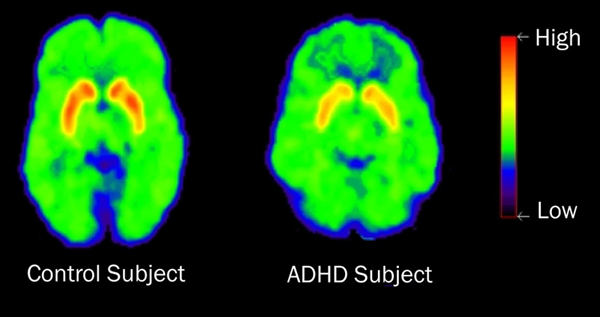
Imagine a life of losing things, of never getting to appointments on time, of not being able to meet one’s own or others’ expectations, of not being able to sustain enduring relationships. Undiagnosed and untreated, Attention Deficit/Hyperactivity Disorder (ADHD) in adulthood can have devastating consequences on the individual’s productivity, employability, family life, social relationships, and general mental and physical health. It is a chronic and usually life-long disorder that influences the individual 24-hours a day. ADHD touches the life of the individual who has the disorder and everyone and everything around him or her.
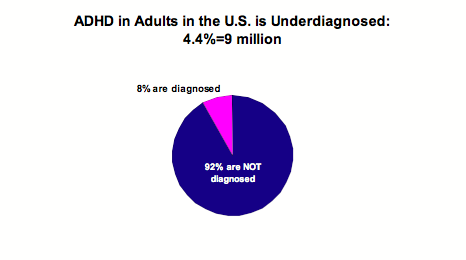
Historically, ADHD has been thought of as a childhood disorder. It was believed that children outgrow the disorder sometime around adolescence. We now know, however, that up to 65% of children with ADHD continue to experience the disorder into adulthood. Recent estimates of prevalence reveal that from 8-10% of children, 9.6% of adolescents, and 4.4% of adults suffer from ADHD.
There are estimated to be about nine million adults with ADHD in the United States and millions more worldwide. It is the challenge to mental health professionals to assist in the identification of the 92% of those adults with ADHD who currently are undiagnosed and to work with other health care providers to offer evidence-based management to improve life success. It is the purpose of this course to present a compelling argument for the importance of identifying ADHD and treating the disorder as early as possible. The extent of the problem will be discussed as well as the complexity in identifying attention problems as a separate disorder in light of the tendency to co-occur with other disorders and obfuscate symptoms. There will be a review of talking therapy approaches and other evidence-based strategies that may be employed by mental health professionals. Accepted medical treatments will be described for informational purposes, since mental health professionals must be abreast of total treatment options. Alternative treatments also will be described.
The Challenges of Adult ADHD
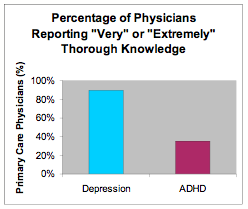
Identifying ADHD in adults has been a significant problem. Why is this? ADHD in adults is not well understood. Until recently, there has been a lack of education, awareness, and acceptance of the diagnosis. This was the case for depression, as well, not long ago. Today, 90% of physicians report having a “very” or “extremely” thorough knowledge of depression compared to a level of understanding of only 35% for adult ADHD. With greater understanding of depression, more adults are receiving appropriate treatment today. With sound education about proper diagnosis and management of ADHD, the same outcomes will be realized for this disorder.
Also, when problems worsen as adults begin independent life, the difficulties often are mistaken for lack of discipline, irresponsibility, or other disorders (depression and anxiety, for example). Screening for ADHD is uncommon in adults and adults commonly underreport the severity of symptoms. Finally, comorbidities are common with ADHD; better-understood conditions are likely to be treated first. Mental health professionals often are called upon to assist in the differential diagnosis of such adults --- to help delineate the symptoms, identify etiology, and suggest a diagnosis or diagnoses --- as initial steps in developing a treatment plan.
The following case, from records of a mental health professional, reflects the difficulty in distinguishing symptoms of ADHD in adults from those of “typical” life stresses or other disorders.
Donna
Donna is 44 years old. She was married for the first time at age 16 to a boy she met in high school. The marriage lasted 17 months. Donna graduated from high school and lived with her mother while she attended a local community college. She then entered a nursing program, during which time she met a young business man. She got married soon after and, with great difficulty and encouragement from her husband, completed nursing school. She became pregnant six months later and two months after taking her first job as a floor nurse at the local hospital.
She was “written up” on many occasions during the 11 months she held the job. She often was late to work, did not keep up with progress notes, and could not seem to follow protocol. Recognizing that her mom and grandmother had been treated for depression and anxiety, she talked with her gynecologist about medication that might help her. However, she was breastfeeding so medication was delayed. She loved the breastfeeding experience and continued until the baby was 16 months old. Then, she started on an antidepressant. However, six months later, Donna was facing likely probation or firing from her nursing job. She stopped taking the medication and decided to have another child and stay home for awhile. She became pregnant the next month. Her husband left during her pregnancy and their divorce followed soon afterwards.
After the baby was born, Donna met Stan and they married six months later. By pooling limited funds, Donna and Stan opened a religious bookstore. They argued often about Donna’s inability to keep up with the books, be at the store on time, and maintain inventory. She was “short” with customers. Bringing the kids to the store, while saving money for childcare, only added more stress to the weak marriage. The store had been in business for about two years when Stan announced that he wanted a divorce and left. Donna decided to continue operating the bookstore, but this lasted just nine months more. While Donna worked hard to be pleasant to employees and customers, she was so overwhelmed by the pressures of the business and family, that she was quickly becoming even more short-tempered. The unpredictability of business also added more pressures. And, being the sole responsible individual for payroll, ordering, opening and closing, and hiring and firing drove the business into a rapid downward spiral. Donna closed the business and returned to what she thought was a more stable and predictable job: being a nurse.
She was hired at a different hospital than the first she had worked. Unfortunately, the problems had not disappeared. She often was late for work and was very disorganized in her work habits --- not a good quality for a nurse in a hospital. When the mental health professional received a call from Donna’s family physician, Donna had been put on probation.
Confusion in Clinical Presentation of ADHD Symptoms
The perception of ADHD as a childhood problem has led to difficulty with its acceptance by the health care field as well as the lay community as an adult problem. This is apparent in the many articles in lay publications and on websites as well as talk show appearances by professionals and others who attribute ADHD-type symptoms to societal ills rather than organic causes. The problem in acceptance of ADHD as an adult disorder is exacerbated by at least two sources.
First, the Diagnostic and Statistical Manual (American Psychiatric Association, 1980, 1987, 1994, 2000) has never included criteria for diagnosing adult ADHD. DSM-II, published in 1968, described only Hyperkinetic syndrome characterized by motoric overactivity. DSM-III, published in 1980, emphasized inattention and suggested that it was possible for some symptoms to persist into adulthood. However, there was no description of adult symptoms. DSM-III-R, published in 1987, recognized the possibility of ADHD in adults with symptoms having to first appear in early childhood. DSM-IV, published in 1994, was the first edition to acknowledge that full ADHD could persist into adulthood, but did not validate the possibility of adult-onset. In fact, it reiterated that symptoms must have appeared prior to age seven. Only in the 2000 edition of DSM-IV-TR were clear references made to adult activities. It discusses impairment in occupational functioning and feelings of restlessness and difficulty engaging in quiet sedentary activities. It should be clear that the Diagnostic and Statistical Manuals, heretofore, have not given a clear acknowledgement to a unique disorder in adults that can guide practitioners in identifying and managing the problem. DSM-V is expected to be published in May of 2012. Expectations are that the new revision will provide the clarification that has been needed.
The second source that interferes with acceptance of adult ADHD is the change in presentation of the disorder with increasing age. It commonly is accepted that the manifestations of the disorder in children include hyperactivity, distractibility, making careless errors, blurting out, interrupting others, difficulty waiting for a turn, and being out of one’s seat at inappropriate times. In fact, the Diagnostic and Statistical Manual identifies a group of symptoms that was developed for children and field-tested using children only (Lahey, et. al., 1994). The current list includes 18 symptoms, nine relating to inattention and nine relating to hyperactivity/impulsivity.
|
Learning Objectives
After completing this course, the mental health professional will be able to
|

is approved by the:
www.psychceu.com
maintains responsibility for the program.
|
All material included in this course is either in the public domain, or used with express permission.
www.psychceu.com adheres to the American Psychological Association's Ethical Principles of Psychologists. Our courses are carefully screened by our Planning Committee to adhere to APA standards. We also require authors who compose Internet courses specifically for us to follow APA ethical standards.
Many of our courses contain case material, and may use the methods of qualitative research and analysis, in-depth interviews and ethnographic studies. The psychotherapeutic techniques depicted may include play therapy, sandplay therapy, dream analysis, drawing analysis, client and therapist self-report, clinical vignettes, etc. The materials presented may be considered non-traditional and may be controversial, and may not have widespread endorsement within the profession. www.psychceu.com maintains responsibility for the program.
Warren Umansky, Ph.D., is a Child Development Specialist in private practice and a school counselor. He has written extensively on child development and special needs topics. His most recent books are ADHD: Helping your child (Warner Books) and Young children with special needs (Merrill Prentice-Hall). He also has developed multimedia programs on ADHD, behavior management, and toilet training, and has published numerous journal articles in scientific and refereed journals.
Dr. Umansky has been a consultant for McNeil Pharmaceuticals and for child care programs, hospitals, and school systems throughout the United States. He is beginning work on another book on ADHD and on a series of children’s books focusing on character education. He lives in Augusta, Georgia with his wife and three children.
Take the test online!
Print out your own certificate!
This course counts as a 'regular' (not self-study) course by the CA BBS!
© 2025. www.psychceu.com. all rights reserved