February 14, 2005
Dear
friends,
I started to write
this when I was honored to be one of the play therapists selected by the
Association
for Play Therapy and OperationUSA to
go to Sri Lanka after the Tsunami to play with children. It was one of
the
most amazing experiences of my life, and I want to thank you for all
the support
you gave me. I continued to write in Sri Lanka, and then, back home,
fueled by jet lag (which I think was really 'soul lag') I kept writing.
And writing. And I may have written too much, so feel free to skip around,
or just look at the pictures.
This is my thank
you to all of you for your support and donations, for the stickers,
band-aids and crayons, for the drawings the children did here, for the
children in Sri Lanka; and to the amazing teams I worked with (from APT:
Janine,
David, Joe, Prabha, Jodi,
Sharolyn,
Valerie,
Maria;
from
OpUSA: Nimmi, Carinne, Ravi and
Anita) and my gratitude to the incredible "animators" of Sri
Lanka, who taught me so much; and to Reverend J. and Selvie-Amah, and
all the children at St. John's orphanage. Most certainly and most especially
my
eternal gratitude to all the wonderful children
and adults
of Sri Lanka who, having survived the war and the Tsunami, opened their
hearts to me.
Thank you forever,
Kate
Kate Amatruda

Tsunami
A
visit to Sri Lanka
A humanitarian mission sponsored
by the Association for Play Therapy and OperationUSA
by
Kate
Amatruda, LMFT, CST-T, BCETS
|

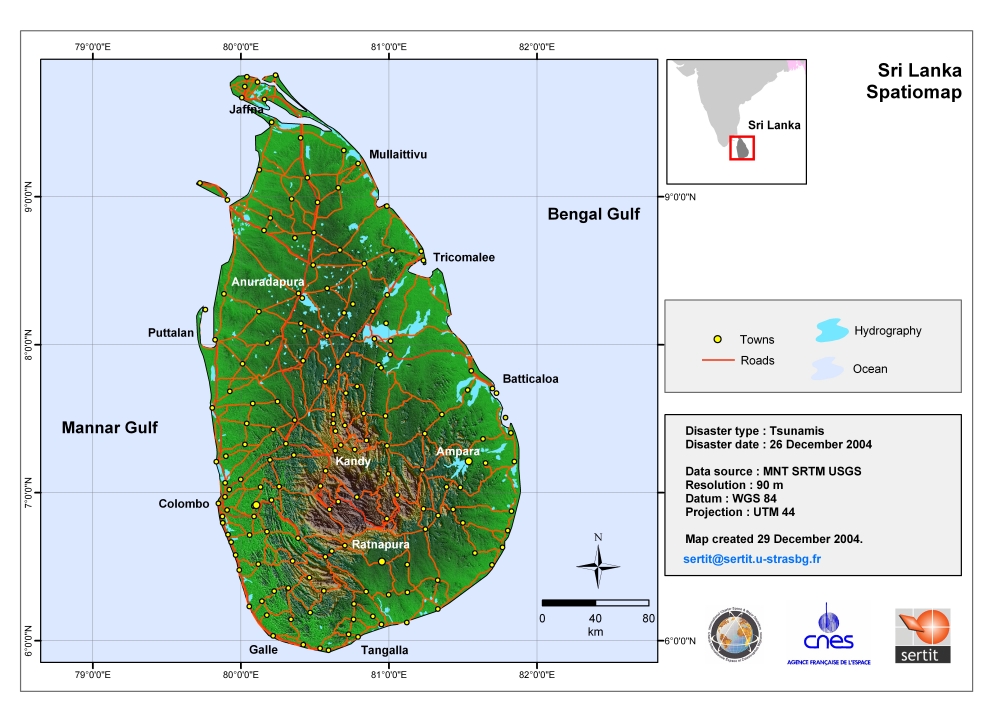
I look on the map and see that Sri Lanka is a teardrop off the coast of India.
I have not slept through the night since I returned from Sri Lanka five
days ago.
It
is
the eyes that haunt me; the eyes of the father whose daughter was ripped out
of his
arms,
the
eyes
of
the
grandmother who saw her children and grandchildren swept away. A generation lost
in a heartbeat. I see shock on the faces of the survivors, and am
reminded
yet again of how everything can change in an instant. Whether it
is an earthquake, a Tsunami, a tornado, or planes hitting towers, life
is so fragile. Everything can be gone in the blink of an eye; we
are so little, nature and war are so big. Yet we have this illusion, at least
in
the
West, that we are in control. So I look, and look again, compelled
to try to discern how people do it. How do you go on when your village,
your home, your family, is destroyed? I see the faces of those who
I met in the refugee camps, and it is the eyes that capture me. And
it
is
the eyes of the children that haunt me, and make me unable to sleep through
the night.
The
number of people believed killed in December's Tsunami disaster rose to 285,993
on Saturday, February 12, 2005. Every day the death toll rises. The number
of children orphaned is still unknown. Sri Lanka's death toll now stands
at 43,832. (Reuters)
The earthquake hit on Sunday, December 26, 2004 at 7:58:53 AM = local time at
epicenter
For us in California, it was on Christmas afternoon,
Saturday, December
25, 2004 at 04:58:53 PM (PST)
Location 3.307° N 95.947° E
Depth 30 km (18.6 miles) set by location program
Region OFF THE WEST COAST OF NORTHERN SUMATRA.
It was a 9.0 earthquake, the fourth biggest since 1900.
(This
should be animated to show the Tsunami. If it is not, try passing your mouse
over the map.
If it does not animate, the non-animated map below shows the
course of the Tsunami.)
I am remembering
the Northern California Loma Prieta earthquake in 1989. The
Indian
Rim "Boxing Day" 9.0 earthquake
makes our 6.9 magnitude pale in comparison,
as
each Richter logarithmically increases the size on an earthquake,
yet the Loma Prieta was strong enough to break the Bay Bridge. Scientists
from Pasadena explain,
"It
has
since
been
shown
to
be proportional to the energy released in the earthquake but the energy
goes up with magnitude faster than
the
ground velocity, by a factor of 32. Thus, a magnitude
6 earthquake has 32 times more energy than a magnitude 5 and almost 1,000
times
more energy than a magnitude 4 earthquake."
"The massive earthquake off the west coast of Indonesia on December
26, 2004, registered a magnitude of nine on the new "moment" scale
(modified Richter scale) that indicates the size of earthquakes.
It was the fourth largest earthquake in one hundred years and largest
since the 1964 Prince William Sound, Alaska earthquake.
The devastating mega thrust earthquake occurred as a result of
the India and Burma plates coming together. It was caused by the
release
of stresses that developed as the India plate slid beneath the
overriding Burma plate. The fault dislocation, or earthquake, consisted
of a
downward sliding of one plate relative to the overlying plate.
The net effect
was a slightly more compact Earth. The India plate began its descent
into the mantle at the Sunda trench that lies west of the earthquake's
epicenter.
For information and images on the Web, visit:
http://www.nasa.gov/vision/earth/lookingatearth/indonesia_quake.html
For the details on the Sumatra, Indonesia Earthquake, visit the
USGS Internet site:
http://neic.usgs.gov/neis/bulletin/neic_slav_ts.html
http://www.nasa.gov/home/hqnews/2005/jan/HQ_05011_earthquake.html
Question: How much energy was released by this earthquake?
Answer: Es 20X10^17 Joules, or 475,000 kilotons (475 megatons)
of TNT, or the equivalent of 23,000 Hiroshima bombs

.
When I get home, I read:
Sumatra Earthquake Three Times Larger Than Originally Thought
EVANSTON, Ill. --- Northwestern University seismologists
have determined that the Dec. 26 Sumatra earthquake that set off a deadly
Tsunami throughout the Indian Ocean was three times larger than originally
thought, making it the second largest earthquake ever instrumentally recorded
and explaining why the Tsunami was so destructive.
By analyzing seismograms from the earthquake, Seth Stein and Emile Okal,
both professors of geological sciences in Northwestern's Weinberg College
of Arts and Sciences, calculated that the earthquake's magnitude measured
9.3, not 9.0, and thus was three times larger. These results have implications
for why Sri Lanka suffered such a great impact and also indicate that the
chances of similar large tsumanis occurring in the same area are reduced.
"The rupture zone was much larger than previously thought," said Stein. "The
initial calculations that it was a 9.0 earthquake did not take into
account what we call slow slip, where the fault, delineated by aftershocks,
shifted
more slowly. The additional energy released by slow slip along the
1,200-kilometer long fault played a key role in generating the devastating
Tsunami.
http://www.sciencedaily.com/releases/2005/02/050211094339.htm
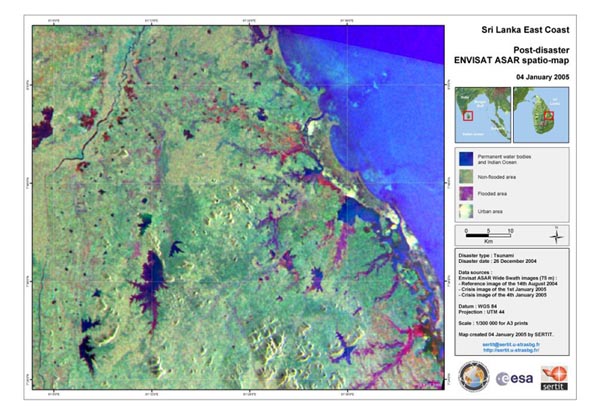
Satellite Imagery

This image acquired on 28 December 2004 by the MERIS (Medium Resolution Imaging
Spectrometer) on board ESA's Envisat Earth observation satellite shows
the northeast coast of Sri Lanka and the southern coasts of India. Sediment
(light
brown & green colour) left after the Tsunami can be seen along the
coast. (Credit: ESA)

Tsunamis
When
thrust-faulting earthquakes happen under the ocean, the earthquake
can push large blocks of ocean floor
up. When the ocean
floor moves up, the water that was in that spot
has to go somewhere else. That somewhere else is into a large wave
called a Tsunami.
http://pasadena.wr.usgs.gov/ABC/pt.html
I
keep feeling there is a "disturbance
on the field"; that something is very wrong.
NASA Details Earthquake Effects on the Earth
NASA scientists using data from the Indonesian earthquake calculated
it affected Earth's rotation, decreased the length of day, slightly
changed the planet's shape, and shifted the North Pole by centimeters.
The earthquake that created the huge Tsunami also changed the
Earth's rotation.
http://www.nasa.gov/home/hqnews/2005/jan/HQ_05011_earthquake.html
Children in the Bay Area of San Francisco, where I live, are
anxious about a Tsunami hitting here. The San Francisco Chronicle has an article
about it, so I am able to reassure my son, as well as myself, that we would
be in no danger. We live on the Petaluma River, but find out that we would
be
protected by the deep channel through the Golden Gate Bridge. Deep harbors
are more able to absorb the shock of a Tsunami than shallow waters.
I received
an e-mail from the Association for Play Therapy calling for a team of volunteers
"to participate in a US delegation to Sri Lanka to provide play activities
(but not psychotherapy) to children in orphanages and community
centers."
I quickly
faxed and mailed off my application, hoping to be selected. I was so honored
when when Dr. Janine Shelby, the Association for Play Therapy Foundation
President, and a brilliant clinician, called to invite me to join the project. I
learned later that only 14 play therapists from across the country have been
selected to go. We will be working with OperationUSA,
an NGO that was the co-recipient
of
the
1997
Nobel
Peace Prize for its work banning land mines. Their mission is based
upon Mahatma Gandhi's belief that "You
must be the change you wish to see in the world".
After
the initial elation, panic sets in. What am I going to do there? I don't
speak the language, nor know the culture. I madly research techniques
for working with children after a disaster, and find very little. There
is a need for Dr. Shelby's project, which will be to bring specific cognitive-behavioral
protocols, in the form of games, to the field.
I find
that the Save the Children guidelines are:
1.Apply
a long-term perspective that incorporates psychosocial well being of
children.
2.Adopt a community-based approach that encourages self-help
and builds on local culture, realities and perceptions
of child development.
3.Promote normal family and everyday life so as to reinforce
a child’s
natural resilience.
4.Focus on primary care and prevention of further
harm in the healing of children’s psychological
wounds.
5.Provide support as well as training for personnel who
care for children.
6.Ensure clarity on ethical issues in order to protect
children.
7.Advocate children’s rights.
I have
ten days notice in which to prepare. I have to tell my patients, and work
through their feelings about me going so soon after the holiday break.
One mother sums it up, "Well, while I am glad for all those children
that you will help, I am not happy for my daughter who you will be leaving!" Shots
- I rush to the doctor to get Hepatitis A and B vaccines, Typhoid, tetanus
and diphtheria shots, and malarial prophylactic pills. After the shots, I
cannot raise my arms for days. I have to pack; we are told to wear long sleeved
shirts (with high cut necklines) and pants. I go to Target and buy loose
fitting
cotton outfits in the pajama department. I will not be a fashion plate this
trip, that's for sure. I spent hundreds of dollars on over-the-counter stuff:
mosquito repellant, sunscreen, tea tree oil, antacids, anti-diarrhea pills,
Advil, Tylenol, anti-itch cream and pills, wipes, toilet paper, hand sanitizer,
etc. I feel like a walking pharmacy.
My
sister, Elizabeth Howell, tells me that one her colleagues and dearest friends
at Calvin College, where they both teach, is from Sri Lanka. His name is
Kumar
Sinniah; he is an Associate Professor in the Department of Chemistry & Biochemistry.
He is wonderful, e-mailing me information, and offering to hook me up with
his five sisters in Sri Lanka. I get helpful e-mails from his sisters Sharmini,
who is working with the Christian Blind Mission, and Melanie.
My one regret was that I was unable to call with them or meet
them when I was in Sri Lanka. When I had a few minutes, finally, on our
last day in Colombo, my laptop, with their phone numbers, went on a little
jaunt through Colombo on its own. Fortunately, it returned intact and in
time for the plane.

To
further prepare, especially emotionally, I go to the Center for Disease Control,
the National Center for Post Traumatic Stress Disorder, and the National
Center for Child Traumatic Stress. (The following articles are in the public
domain. Feel free to skip them if you just want to read about my journey.)
Disaster Rescue and Response Workers
A National Center for PTSD Fact Sheet
The terrorist attacks on New York and Washington are, together, the greatest
man-made disaster in America since the Civil War. Lessons learned from
natural and human-caused disasters can help us understand the unique stressors
faced by rescue workers such as police and firefighters, National Guard
members, emergency medical technicians, and volunteers. Past experience
may also help us recognize how these stressors may affect response
workers. Rescue workers face the danger of death or physical injury, the
potential loss of their coworkers and friends, and devastating effects
on their communities. In addition to physical danger, rescue workers are
at risk for behavioral and emotional readjustment problems.
What psychological problems can result from disaster experiences?
The psychological problems that may result from disaster experiences include:
- Emotional reactions: temporary (i.e., for several days or a couple
of weeks) feelings of shock, fear, grief, anger, resentment, guilt, shame,
helplessness, hopelessness, or emotional numbness (difficulty feeling
love and intimacy or difficulty taking interest and pleasure in day-to-day
activities)
- Cognitive reactions: confusion, disorientation, indecisiveness, worry,
shortened attention span, difficulty concentrating, memory loss, unwanted
memories, self-blame
- Physical reactions: tension, fatigue, edginess, difficulty sleeping,
bodily aches or pain, startling easily, racing heartbeat, nausea, change
in appetite, change in sex drive
- Interpersonal reactions in relationships at school, work, in friendships,
in marriage, or as a parent: distrust; irritability; conflict; withdrawal;
isolation; feeling rejected or abandoned; being distant, judgmental,
or over-controlling
What severe stress symptoms can result from disasters?
Most disaster rescue workers only experience mild, normal stress reactions,
and disaster experiences may even promote personal growth and strengthen
relationships. However, as many as one out of every three rescue workers
experience some or all of the following severe stress symptoms, which may
lead to lasting Posttraumatic Stress Disorder (PTSD), anxiety disorders,
or depression:
- Dissociation
(feeling completely unreal or outside yourself, like in a dream; having "blank" periods
of time you cannot remember)
- Intrusive reexperiencing (terrifying memories, nightmares, or flashbacks)
- Extreme attempts to avoid disturbing memories (such as through substance
use)
- Extreme emotional numbing (completely unable to feel emotion, as if
empty)
- Hyper-arousal (panic attacks, rage, extreme irritability, intense agitation)
- Severe anxiety (paralyzing worry, extreme helplessness, compulsions
or obsessions)
- Severe depression (complete loss of hope, self-worth, motivation, or
purpose in life)
Who is at greatest risk for severe stress symptoms?
Rescue workers who directly experience or witness any of the following
during or after the disaster are at greatest risk for severe stress symptoms
and lasting readjustment problems:
- Life threatening danger or physical harm (especially to children)
- Exposure to gruesome death, bodily injury, or dead or maimed bodies
- Extreme environmental or human violence or destruction
- Loss of home, valued possessions, neighborhood, or community
- Loss of communication with or support from close relations
- Intense emotional demands (such as searching for possibly dying survivors
or interacting with bereaved family members)
- Extreme fatigue, weather exposure, hunger, or sleep deprivation
- Extended exposure to danger, loss, emotional/physical strain
- Exposure to toxic contamination (such as gas or fumes, chemicals, radioactivity)
Studies also show that some individuals are at a higher than typical risk
for severe stress symptoms and lasting PTSD if they have a history of:
- Exposure to other traumas (such as severe accidents, abuse, assault,
combat, rescue work)
- Chronic medical illness or psychological disorders
- Chronic poverty, homelessness, unemployment, or discrimination
- Recent or subsequent major life stressors or emotional strain (such
as single parenting)
Disaster stress may revive memories of prior trauma and may intensify
preexisting social, economic, spiritual, psychological, or medical problems.
How can you manage stress during a disaster operation?
Here are some ways to manage stress during a disaster operation:
Develop a "buddy" system
with a coworker.
Encourage and support your coworkers.
Take care of yourself physically by exercising regularly and eating small
quantities of food frequently.
Take a break when you feel your stamina, coordination, or tolerance for
irritation diminishing.
Stay in touch with family and friends.
Defuse briefly whenever you experience troubling incidents and after each
work shift.
How can you manage stress after the disaster?
After the disaster:
- Attend a debriefing if one is offered, or try to get one organized
2 to 5 days after leaving the scene.
- Talk about feelings as they arise, and be a good listener to your coworkers.
- Don't take anger too personally - it's often an expression of frustration,
guilt, or worry.
- Give your coworkers recognition and appreciation for a job well done.
- Eat well and try to get adequate sleep in the days following the event.
- Maintain
as normal a routine as possible, but take several days to "decompress" gradually.
How can you manage stress after returning home?
After returning home:
- Catch up on your rest (this may take several days).
- Slow down - get back to a normal pace in your daily life.
- Understand that it's perfectly normal to want to talk about the disaster
and equally normal not to want to talk about it; but remember that those
who haven't been through it might not be interested in hearing all about
it -they might find it frightening or simply be satisfied that you returned
safely.
- Expect disappointment, frustration, and conflict -sometimes coming
home doesn't live up to what you imagined it would be -but keep recalling
what's really important in your life and relationships so that small
stressors don't lead to major conflicts.
- Don't be surprised if you experience mood swings; they will diminish
with time.
- Don't overwhelm children with your experiences; be sure to talk about
what happened in their lives while you were gone.
- If talking doesn't feel natural, other forms of expression or stress
relief such as journal writing, hobbies, and exercise are recommended.
Taking each day one at a time is essential in disaster's wake. Each day
provides a new opportunity to FILL-UP:
* Focus Inwardly on what's most important to you and your
family today;
* Look and Listen to learn what you and your significant
others are experiencing, so you'll remember what is important and let go
of what's not;
* Understand Personally what these experiences mean to you,
so that you will feel able to go on with your life and even grow personally.
______________________________________________________________________________
Psychological Impact of the Tsunami Across the Indian Rim
National Child
Traumatic Stress Network
www.NCTSNet.org
The massively
destructive Tsunami that struck across the Indian Rim caused
extensive loss of life and injury as well as devastation to property
and community
resources. The combination of life-threatening personal experiences,
loss of loved ones and property, massive disruption of routines and
expectations
of daily life, pervasive post-disaster adversities, and enormous
economic impact on families and entire nations pose an extreme psychological
challenge
to the recovery of children and families in the affected areas.
This brief information sheet provides an overview of expected psychological
and physical
responses among survivors. The key concepts include:
o
Reactions to Danger
o
Posttraumatic Stress Reactions
o Grief Reactions o Traumatic Grief o
Depression
o Physical Symptoms o Trauma and Loss Reminders
o Post-disaster
Adversity/Disruption
Appreciating
the psychological implications of such an overwhelming event on the lives
of the survivors plays a crucial role
in considering specific efforts that will be of greatest help to the
affected
communities. The following issues may be helpful to consider in efforts
to respond to disaster victims:
Reactions
to Danger
It
is important to recognize the difference between a sense of danger and
reactions to
traumatic
events. Danger refers to the sense that events or activities have
the potential to cause harm. In the wake of the recent disaster, people
and communities
have greater appreciation for the enormous danger of a Tsunami
and the need for an effective early warning system. There are likely
to
be
widespread
fears of recurrence that are increased by misinformation and rumors.
Danger always increases the need and desire to be close to others,
making separation
from family members and friends more difficult.
Posttraumatic
Stress Reactions
These
reactions are common, understandable, and expectable, but are nevertheless
serious and can lead to many difficulties in daily life. There
are three types of posttraumatic stress reactions. Intrusive Reactions
are ways
the traumatic experience comes back to mind.
These
include:
o
recurrent
upsetting
thoughts or images that occur while awake or dreaming
o
strong emotional or physical reactions to reminders of the Tsunami
o
feelings
and
behavior as if something as terrible as the Tsunami
is happening again
Avoidance
and Withdrawal Reactions include:
o
avoiding talking, thinking, or having feelings about the Tsunami
o avoiding
places and
people
connected to
the event
o feeling emotionally numb, detached
or estranged from others
o
losing interest in usually pleasurable activities
Physical Arousal Reactions are
physical changes that make the
body react as if danger is
still present.
These
include:
o
constantly being “on
the lookout” for danger
o being startled easily or being jumpy or
nervous
o feeling ongoing irritability or having outbursts of anger
o
having difficulty falling or staying asleep or having restless, easily
disturbed sleep
o having difficulty concentrating or paying attention
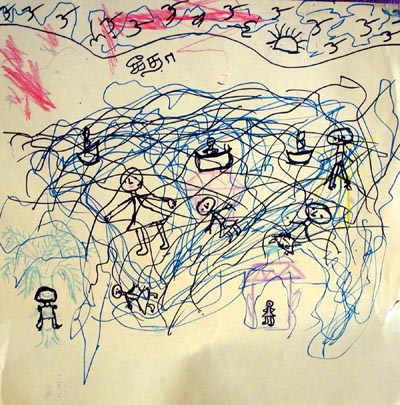
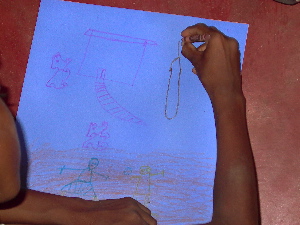
Children
may show some of these reactions through their play or drawing. They
may have bad dreams that are not specific to the Tsunami. In addition
to increased irritability,
children may also have physical complaints (headaches,
stomachaches, vague aches
and pains). Sometimes these are difficult to distinguish from true
medical concerns.
Grief
Reactions
Those
who survived the Tsunami have suffered many types of losses – including
loss of loved ones, home, possessions, and community. Loss may lead to:
o
feelings of sadness and anger
o guilt or regret over the loss
o missing
or longing
for the deceased
o
dreams of seeing the person again
These
grief reactions are normal, vary from person to person, and can last
for many years after
the loss. There is
no single “correct” course of grieving.
Personal, family, religious and cultural factors affect the course of grief.
Although grief reactions may be painful to experience, especially at first,
they are healthy reactions and reflect the ongoing significance of the
loss. Over time, grief reactions tend to include more pleasant thoughts
and activities, such as positive reminiscing or finding positive ways to
memorialize or remember a loved one. One of the many untoward results of
the Tsunami is that some family members’ bodies
have not been found. This,
unfortunately, has prevented
the normal use of religious,
and cultural
burial and mourning rituals,
and has put
the experience of grief
on hold. Whereas trauma
is more restricted to
personal experience of
the Tsunami, loss and grief
extend well beyond the
impacted
areas, indeed across the
world.
Traumatic
Grief
People
who have suffered the traumatic
loss of a loved
one often find grieving more difficult.
Their minds stay
on the circumstances
of the death,
including preoccupations
with how the loss could have been
prevented, what
the last moments
were like, and issues of accountability.
These reactions
include:
o intrusive, disturbing
images of the
manner of death that interfere with
positive remembering
and reminiscing
o delay in the onset of healthy
grief reactions
o retreat from close relationships
with
family and friends,
and avoidance of usual activities
because they
are reminders of the traumatic loss
Traumatic
grief changes
the course of mourning, putting
individuals
on a different time course than is usually
expected by
other family members, religious rituals,
and cultural
norms that offer support
and comfort.
Depression
Over
time, the risk of depression after the Tsunami is an additional
major concern. Depression is
associated
with prolonged grief and strongly related
to the
accumulation of post-Tsunami adversities.
Symptoms
include:
o persistent depressed or irritable
mood
o
loss of appetite
o sleep
disturbance,
often
early morning
awakening
o
greatly
diminished
interest
or pleasure
in
life
activities
o fatigue
or loss
of energy
o feelings
of worthlessness
or guilt
o feelings
of hopelessness,
and sometimes
thoughts
about
suicide
Demoralization is a common
response
to acutely
unfulfilled
expectations
about
improvement in
post-disaster
adversities,
and resignation
to adverse
changes
in life circumstances.
Physical
Symptoms Survivors
of
the Tsunami may experience
physical
symptoms,
even
in the absence
of
any underlying physical
injury
or illness.
These
symptoms include:
o
headaches, dizziness
o
stomachaches,
muscle
aches
o rapid
heart
beating
o
tightness
in
the chest
o
loss
of appetite
o bowel
problems
In
particular,
near-drowning
experiences
can
lead to panic
reactions,
especially
in
response to reminders.
Panic
often
is expressed
by
cardiac, respiratory,
and
other physical
symptoms.
More
general anxiety
reactions
are
also to
be
expected. Physical
symptoms
often
accompany posttraumatic
grief
and depressive
reactions.
More
generally, they
may
signal
elevated
levels
of life
stress.
Trauma
and Loss Reminders
Posttraumatic stress
reactions are
often evoked
by trauma reminders.
Many people
continue to encounter
places, people,
sights, sounds, smells, and
inner feelings that remind
them of the Tsunami experience.
The ocean
has become
a powerful
reminder. Additionally,
the tide simply
going out or
even the wave in
a bathtub
while bathing
a child can
act as a
disturbing reminder.
Because the Tsunami was
accompanied by
a loud
roar and
the crashing of waves,
loud noises can be
strong reminders.
Reminders can
happen unexpectedly, and it can
take quite a while
to calm down
afterward. Adults
and children are often
not aware that
they are responding
to a
reminder, and
the reason
for their
change in mood
or behavior may go
unrecognized. The day of
the week, the time
of day,
and the anniversary
date are common
reminders. Television
and radio news
coverage can
easily serve
as unwelcome reminders.
It is particularly difficult
when family
members have been
together during
a traumatic experience,
because afterward
they can serve
as trauma reminders
to each other, leading to
unrecognized disturbances
in family relationships.
Grief
reactions are often
evoked by loss
reminders. Those
who have lost
loved ones
continue to
encounter situations
and circumstances that
remind them of
the absence
of their loved
one. These reminders
can bring
on feelings
of sadness, emptiness
in the
survivor's life,
and missing
or longing for
the loved one's
presence.
There
are several types
of loss reminders: Empty
situations occur
when one would
be used to being with
a loved one
and they are no longer
there, for
example at the
dinner table,
during activities
usually done together,
and on special occasions,
like birthdays and holidays.
Children, adolescents,
and adults
also are
reminded by
the everyday changes
in their lives,
especially hardships
that result from
the loss.
Examples include
temporary or changed
caretakers, decreases
in family income,
depression and
grief reactions
in other family
members, disruptions
in family functioning,
increased family
responsibilities, lost
opportunities (for example,
sports, education, and
other activities),
and the loss of a sense
of protection
and security.
Post-disaster
Adversities/Disruption
Successfully
addressing the
multitude of post-disaster
adversities not
only saves lives,
protects health,
and restores
community function,
but constitutes an important
mental health intervention.
Contending with
adversities such as
lack of shelter,
food and other resources,
and disruption
of daily routines
can significantly deplete
coping and
emotional resources
and, in
turn, interfere with recovery
from posttraumatic
stress, traumatic
grief, and
depressive reactions.
Post-disaster medical
treatment and
ongoing physical rehabilitation
can
be another
source of
post-disaster stress.
New or
additional traumatic
experiences and
losses after
the initial
experience are
known to
exacerbate distress
and interfere
with recovery.
Likewise, distress
associated with
prior traumatic
experiences or
losses can
be renewed
by the
experience of
the Tsunami.
Children’s
recovery is put in jeopardy without proper caretaking, reunification
with family members, and restoration of normal daily routines – for
example, schooling. Some adversities require large-scale responses,
while others
can be addressed, in part, by personal and family problem solving.
What
Are the Consequences of These Reactions?
Post-disaster
reactions can be
extremely distressing and may significantly interfere with daily activities.
For adults, posttraumatic stress, grief, and depressive reactions
can impair effective decision-making, so vital in adapting to the recovery
environment.
They also compromise parenting. For children and adolescents, intrusive
images and reactivity to reminders can seriously interfere with learning
and school performance. Worries and fears may make it difficult for
young children to return to school or to venture any distance
from parents or
caregivers.
Avoidance
of reminders can lead adolescents to place restrictions
on important activities, relationships, interests and plans for the
future. Irritability can interfere with getting along with family
members and friends.
Trauma-related sleep disturbance is often overlooked, but can be especially
persistent and affect daytime functioning. Adolescents and adults
may respond to a sense of emotional numbness or estrangement by using
alcohol or drugs.
They may engage in reckless behavior. Adolescents may become inconsistent
in their behavior, as they respond to reminders with withdrawal
and avoidance or overly aggressive behavior. Over time, there may
be increases in marital
discord and domestic violence.
Depressive
reactions can become quite serious, leading to a major decline in school
or occupational
performance
and learning,
social isolation, loss of interest in normal activities, self-medication
with alcohol or drugs, acting-out behavior to try to mask the depression,
and, most seriously, attempts at suicide.
Traumatic
grief can lead to the inability to mourn, reminisce and remember, fear
a
similar fate or the
sudden loss of other loved ones, and to difficulties in establishing
or maintaining new relationships. Adolescents may respond
to
traumatic
losses
by trying to become too self-sufficient and independent from parents
and other adults, or by becoming more dependent and taking
less initiative.
Coping
after Disaster
In
addition to meeting peoples basic needs for food,
water, shelter, clothing and medicine, there are several ways to enhance
people’s
coping. Physical:
Stress can be
reduced with
proper nutrition,
exercise and sleep.
People may need
to be reminded
that they
should take
care of themselves
physically to
be of help
to families and communities.
Emotional:
People need
to be reminded
that their
emotional reactions
are normal and expected,
and will decrease
over time.
However, if their
reactions are too
extreme or do
not diminish
over time,
there are professionals
who can be of
help. Social:
Communication with,
and support from,
family members,
friends, religious
institutions and the
community are very
helpful in coping
after a disaster.
People should
be encouraged to communicate
with
others, and to
seek and use
this support
where available.
Daily
Routines:
For children especially,
it is important
to restore
normal routines,
including mealtimes,
bedtime) as much
as possible. Children
feel more
safe and secure
with structure
and routine. Meeting
basic survival
needs, restoring
a sense of safety
and security, and providing
opportunities
for normal development
within the social,
family and community
context are important
steps to
the recovery of children
and adolescents.
source:
http://www.nctsnet.org/nccts/asset.do?id=603
This
project was funded
by the Substance
Abuse and Mental
Health Services
Administration (SAMHSA),
US Department of Health
and Human Services
(HHS). The views,
policies, and
opinions expressed
are those of the
authors and do
not necessarily reflect
those of SAMHSA
or HHS.
My
preparation to go to Sri Lanka was aided by a visit to Leland "Skip" and
Aew Whitney, Mill Valley residents who arrived in Colombo just after the
Tsunami. Synchronistically, Skip is on the board of OperationUSA; I read
about his family's journey in the local paper and then called him. He and
his wife graciously invited me to their home to tell me about what had happened
to them.
Mill Valley man helps in Tsunami zone
Jason Walsh, IJ reporter
Wednesday, January 19, 2005
- As a fund-raising board member of the international relief foundation
OperationUSA, Skip Whitney is used to helping disaster victims from a
distance.
But when fate placed the Mill Valley real estate developer at the center
of the Sri Lankan Tsunami devastation, Whitney found himself offering relief
in ways he never would have imagined. Whitney, his wife, Aew, and their
two daughters were vacationing in Southeast Asia during the holidays and
were due to fly from Bangkok to Colombo, Sri Lanka on Christmas Day. But,
because of a miscalculated departure time, the Whitneys missed their flight
- as well as the earth-shattering waves that rocked the island the next
day. "I have no doubt in my mind that if we had arrived on schedule,
we would be dead," Whitney said. Having heard only vague rumors of
a tidal wave and unaware of the full extent of the catastrophe, the Whitneys
caught the next flight to Colombo, arriving hours after the Tsunami swept
away the lives and homes of thousands of Sri Lankans. (The full story is
at http://opusa.org/press/marin_ind.htm)
As I prepare to go to Sri Lanka, I also solicit donations from friends
and the local schools. It is so hard to ask for money that instead
I ask for
crayons,
paper, scissors,
stickers, and children's band-aids. People are wonderful. Especially
moving are
the letters and drawings done by children here to give to
children in Sri Lanka. People I did not know were coming up to me, offering me crayons,
blessings,
good wishes, and respect. It is the admiration that throws me, as I
feel this is something I have to do; a call I must answer.

Friday, January 28, 2005
Today
is my flight, and at 4:00 a.m., I am still awake.
The alarm is set for 5:00 a.m. to begin the journey. Yet here I am,
packing and
racing around, fueled by adrenaline, anxiety and pressure to get everything
into one small bag. I am
shocked by my lack of preparation; why am I just now starting to pack? It
was hard, I had only known for a week and one half that I was going to Sri Lanka, and only found out yesterday I will be in the group going to Batticaloa,
affectionately known as “Batti”. I hear many jokes from my son
Colety that “Mom is going Batty!”, which feels very true at the
moment. We are allowed two bags, up to 70 lbs each, so my husband
Roy and son Colety packed the big suitcase with things for the children:
stickers, paper, letters and drawings from children here, zillions of children’s
band-aids, scissors, paper punches and balloons. 69 pounds, all donated.
Colety handed me a roll of money; between bake sales and
spare change
jars, the Novato Charter School had collected $200 for
the children of Sri Lanka.
7:09
am
Now the journey really begins. I missed the Airporter bus, so Roy had to race
me to the Larkspur terminal to catch another bus. Kate Chaos! I do get a little
tired of my frenzy at times, wishing for some of Roy's composure and serenity.
Finally, I am on the Airporter bus, heading to SFO. From there, I catch a plane
to LA,
switch airlines
and terminals, meet with the group, and then we fly
to Colombo, via
Tokyo and Singapore.
Our
team met in boarding area of Singapore Airlines, we range in age from 26
(our leader,
David) to the geriatric
one among us; me, age 50. We
bring a wide range of experience to the project. We will
find out more of what we will be doing in Singapore;
there
will
be training.
The
interventions
are specific, and directive. We cannot bring
anything aquatic, including in the stickers.
I would like to know
more about this;
it seems a paradox to
be directive, but avoid talking about the thing that
caused the trauma. Kind of the "you-know-who" Lord Voldemort
thing in Harry Potter.
We had received an e-mail from the Association for Play Therapy; our team is:
Janine
Shelby, Ph.D., B.C.E.T.S., RPT-S is a licensed psychologist and a clinical
faculty member
in the department of Psychiatry at UCLA. When she returns from Sri Lanka, she
will assume the position of Chief Psychologist in the Child Crisis Center,
Department of Pediatrics, Harbor-UCLA Medical Center. She is a frequent consultant
for OperationUSA and other NGOs, a consultant for the National Center for
Child Traumatic
Stress, and a long-term American Red Cross volunteer. She appears on the National
Red Cross mental health training video. Dr. Shelby has lectured in and provided
relief to survivors in more than a dozen countries including those in the former
Yugoslavia, Russia, Western Europe, Asia, and Latin America. Her articles and
book chapters focus on posttraumatic interventions for traumatized children.
She is the President of the Foundation for the APT and in that capacity, worked
with OperationUSA, the Foundation Board, APT staff to design the project in
which we are participating.
Our
leader, David Bond MSW, has been collaborating with the National Center for
Child Traumatic Stress for the last nine months on Psychological First
Aid, an early response intervention protocol to be used in the immediate
aftermath of terrorist attacks and natural disaster. He works full time as
a psychotherapist at St. Francis Medical Center in Lynwood, CA. David
is a member of APT and has completed the requirements for the RPT credential,
for which he will apply upon obtaining his LCSW in March '05. He is currently
co-authoring a chapter on mental health practitioners' involvement in post-disaster
relief work.
Kate
Amatruda, MA, LMFT, Novato, CA: UC Berkeley Adjunct Faculty, Certified Sandplay
Therapist-Teacher, relief work during Loma Prieta Earthquake, 9/11 work in
schools, ARC Disaster Mental Health Member, CAMFT Trauma Response Network
Responder, Author of "Trauma, Terror and Treatment: PTSD in Children
and Adults".
Sharolyn Wallace Bowman, Ph.D. (Social Work), Tulsa, OK:
Professor at Tulsa Community College, 18 experience
in the childhood
grief field,
past experiences
working
in Russian orphanages doing related work, RPT-S (Registered
Play Therapist-Supervisor), Officer for OK Branch of
the APT
Valerie Hearst, LGSW, Brunswick, OH: Provided work to orphanage in Mexico
and Standing Rock Reservation, lived and studied in Mexico, social justice
trip to Puerto Rico and Dominican Republic, backpacked in Thailand, Mexico,
Guatemala, and Belize
Maria Parreno, Psy.D., Psychologist, Mission Viejo, CA:
Experience with relief work after Hurricane Iniki,
volunteer work in
orphanages in Mexico,
studied
in Israel during war, background growing up in Philippines
with missionary parents
Prabha Sankaranarayan, MS (Child Development), Pittsburgh,
PA: Therapist and Mediator, Snyder & Sankar Associates, 20 years experience working
with children, lived in India for 20 years, speaks Tamil (one of the
Sri Lankan languages),
NOVA training, currently writing PA plan for victims of a terrorist
attack
Jodi Smith, LCSW, Claremont, CA: social worker at Children’s
Hospital LA in ER and long-term wards for crisis and
trauma victims, Red Cross Volunteer, provided recreational
activities for orphans in Mexico
Joseph Wehrman, Ph.D. (Counselor Education), Aberdeen,
SD: Many years experience working in early childhood,
former member of
US Army where
he provided
on-site medical care to remote villages in Honduras,
lived and worked in Iraq providing
medical care to civilians and soldiers, worked 5 years
in
early childhood development, former Hall Director for
international students.

clockwise:
Kate, Joe, Prabha, Jodi, Sharolyn, David, Valerie, Janine and Maria
The
flights are endless. We left LA at 1:00 pm, went to Tokyo for a refueling.
In Tokyo, even though the layover was less than an hour,
everyone had to get off the plane, exit, go through security again,
wait in a long line, and get back on the plane. The security guards,
the ones who run your things through the x-ray machines, are all young
women, wearing red hats, red skirts and vests, with white blouses.
They wear high heels, as does every Japanese woman we see who works in the
airport. All the people I
encounter on the plane, in the airports, even at the security screening areas
are so touched that I am
going to
Sri Lanka,
that they
thank me. I accept their gratitude,
knowing it is soul food that will sustain me during the hard times.
The
LA to Tokyo flight was 11h 40m long. Tokyo to
Singapore is 7h 30m long. Singapore to Colombo 3h 35m. 22 hours and 45 minutes
in airplanes! Are we there
yet?
Back on the plane, seven+ more hours in the air until Singapore. I am getting
a bit squirrelly. It would be nice to go outside, breathe fresh air. In
Singapore, we stagger out of the airport, having been stamped through
immigration
(I was so happy to get a stamp in my new passport) and through the “nothing
to declare” line in customs. We get off the plane, into the
night, and realize we have no way of getting to the hotel. David
arranges
for a van, and we get to the hotel at 3:00 a.m., but which day I
have no idea.
Sunday
Hotel, shower, sleep. In the morning, David tells us “The Protocol”,
a series of exercises designed by Janine Shelby and her team to help
children master trauma. They are cognitive behavioral, with specific objectives
and
techniques. Each game has the objective, such as to:
*Normalize
reactions ("Yes, you are having a 'normal' reaction to
an 'abnormal' situation; whatever you are experiencing;
sleep difficulties, crying, anger, etc. is OK and normal."
In my work in the States, this is the stage
when I usually reassure a person that they are NOT crazy,
but
in Sri Lanka I don't know the cultural context for craziness.)
*Assess current coping mechanisms (and reinforce healthy ones),
*Assess and modify misattributions and cognitive distortions (such
as if the child feels that he or she did something
to cause the Tsunami)
*Decrease hyperarousal and panic symptoms (We hear that at one camp,
people feared that another Tsunami was coming. Some children were hurt
in the
stampede.)
*Increase self-soothing (breathe! breathe!)
*Identify and change intrusive re-experiencing, such as flashbacks
*Decrease isolation
and withdrawal and reinforce the ability to seek helpful
social support (ask for a hug, find someone to talk to, tell a grown-up)
*Decrease regressive behaviors by focusing on strengths and resources
*Identify loss reminders (water images, perhaps the aquatic stickers?)
and trauma triggers (such as loud noises, big waves, whatever you were
doing at
the time
at the
disaster)
*Finally,
to leave
the child with a sense of hope.
(Adapted from "Enhancing Coping Among
Young Tsunami Survivors: Culturally Approved Interventions
1/24/05 © Shelby,
Bond, Hall & Hsu, 2004)
I am
worried that our attempts to help will come to nothing; that we are offering
a band-aid for a gaping wound. A disaster that has killed so many cannot
be quickly overcome, particularly after so much war trauma.
The Tsunami is a holocaust that will affect Sri Lanka, the Indian Rim nations,
and the world for generations. And no technique will work if the hierarchy
of needs is not met; if the child is still in danger, hungry, or without
shelter. The first step in trauma work is to establish that the danger is
over, that the child is safe now.
Child
Trauma Intervention Model
Click
here for a power point presentation published by The National Resource
Center for Child Traumatic Stress, and adapted from:
Pynoos RS, Goenjian AK, Steinberg AM: (1998) A public mental health
approach to the post-disaster treatment of children and adolescents.
Psychiatric Clinics of North America 7:195-210.
Psychological
First Aid
Click
here for a power point presentation published by The National Resource
Center for Child Traumatic Stress, and adapted from: Pynoos RS, Nader
K: (1988) Psychological first aid and treatment approach to children
exposed to community violence: Research implications. Journal of
Traumatic Stress 1: 445-473. These
ideas are the basis of the techniques we used in Sri Lanka.
|
Why do we go
to play, and teach play techniques, in a cataclysm? As we get closer
to Sri Lanka, my mind struggles to
hold
the number who died. September 11 was about 3000, the Tsunami
was around 150,000 when I left. By the time I returned home the death
toll was 285,000; the count rises each day. I think we go to play with children
because play
is the first language, before children can verbalize, they play. Play allows
for the expression and healing of trauma. And we go because we, as humans,
want to do something for other humans who are suffering.
After working all day in Singapore, we have a few hours off. Prabha,
Valerie and I jump into a cab and go to Chinatown. We walk through
crowded streets; Chinese New year is almost here, so it is very
festive. Great shopping; I keep thinking I could make a killing
on EBay if
I had enough time and money, connections, and could carry everything.
This
must be how people make money; they buy things very cheaply,
sell high. What an alien concept for a therapist! Not this lifetime!
We check
out of the hotel and then leave for the airport to head
to Colombo, the biggest city in Sri Lanka. We
had arrived at the hotel
at 2:00 a.m., and we leaving at 8:00 p.m. the same day...how
many hours is that? 18 hours, most of it spent in training.
We
get to Colombo, where there is a strong military presence. The Army
is everywhere, running checkpoints and randomly pulling over
cars. We are pulled over and the soldiers shine a flashlight into
the car, mostly focusing
on Valerie. She is scared, keeps asking, “Should
I open the door?” Everyone
yells out, “No! No!” Later we find out we
were stopped because some of the women in our group have
short hair. The women fighters of the Liberation Tigers
of Tamil Eelam (LTTE), or Tamil Tigers,
are the only women in this country to have short hair. We
get to the hotel very late, it is 3:00 a.m. I am still awake,
wondering what is to come.
Monday
The next day is Monday, and we have another meeting, this time with Nimmi Gowrinathan,
an  OperationUSA worker,
a tall, brilliant and gorgeous Tamil woman who grew up in Los Angeles,
and is getting a Ph.D. in Political Science
from UCLA. She embodies her quote, "Leadership
is the capacity to translate vision into reality." Nimmi
orients us to the political and social structure of the country.
We learn about the
years of warfare, the riots, the discrimination
that the Tamil have felt at the hands of the Singhalese. (For more on this
conflict, please go to: Sri
Lanka: Ethnic Conflict & Civil War.)
OperationUSA worker,
a tall, brilliant and gorgeous Tamil woman who grew up in Los Angeles,
and is getting a Ph.D. in Political Science
from UCLA. She embodies her quote, "Leadership
is the capacity to translate vision into reality." Nimmi
orients us to the political and social structure of the country.
We learn about the
years of warfare, the riots, the discrimination
that the Tamil have felt at the hands of the Singhalese. (For more on this
conflict, please go to: Sri
Lanka: Ethnic Conflict & Civil War.)
There
is now a cease-fire in the war. We
learn that three days after we left Batticaloa that Kousalyan, the head
of the
Liberation
Tigers'
political
division
for the Batticaloa-Amparai district, was killed in an ambush
on the highway to Batticaloa Monday night February 7 around 7:45. Three
people who were traveling with him were killed and four were injured.
[source: TamilNet,
February 07, 2005 16:08 GMT]
I
wonder how this will affect the survivors of the Tsunami...how can they
begin to feel safe if the war comes again? I
cannot help but feel we left just in time, and, after viewing the devastation
wrought by nature, I would like
to bring the leaders of every country to view it, to tell them to
stop all wars. To help rebuild the planet. To stop senseless killing. To
use resources to end human suffering, not to increase it. (Of course,
I do keep all these sentiments to myself. One of the requirements of disaster
response
is to
be non-political,
non-denominational and nondiscriminatory.
We offer aid by need, not religion, ethnicity, political affiliation,
etc.)
We
have two teams, one headed to the South, the area that is primarily Buddhist
and Singhalese. My
team's destination is Batticaloa,
ground
zero
of
the
Tsunami,
and the place where there have been the least services provided. The East
is primarily Tamil, with the major religions being Hindu and Muslim. There
also seem to be pockets of Christianity throughout the country, and
the Eastern team will be staying at an orphanage started by Christian Missionaries.
We learn about the social customs; that women tie their hair up
or back at all times, that dress is modest,
with most
of the body covered. Women and girls wear earrings, and we hear
tales that if a woman has a hole in her ear, without an earring in it,
that the
Sri
Lankan
women will come
up and try to put an earring in the piercing. Irreverently we joke that
is a way to get more earrings. The henna paintings on hands, toe
rings and lovely sandals make sense if a woman's body is mostly covered;
for where else can she show her beauty?
We then briefly meet Janine Shelby, the play therapist who has
masterminded this project. She is very busy in Colombo, doing
many trainings. David asks
her some clarification questions and then she ends by giving us some
lovely words of encouragement for our mission. We race upstairs to
pack
up the
toys, and we are off to Batti, while the southern team heads toward Galle.

To Batticaloa is a long drive, at least 8 hours through the center of the
island. The roads are winding, the countryside incredibly  beautiful.
We see
elephants and monkeys, and go by some huge statutes of
the Buddha, towering over the town and countryside.
beautiful.
We see
elephants and monkeys, and go by some huge statutes of
the Buddha, towering over the town and countryside.
We are
regretting the ‘typical Sri Lankan breakfast’ of
very spicy curry we had this morning, as it is raising havoc
with our Western tummies. For bathrooms, we stop at “rest houses”,
which have little cafés with bathroom facilities. Almost
all have ‘English toilets’, but not all. The alternative
is a hole in the ground over which one squats. You stand on
little wooden
steps, pull your pants down and to the front, and squat down
low, trying not to splash yourself. There is a bucket of water
nearby that you
fill and dump in quickly, hoping to flush. We carry our own
toilet paper, as few rest houses have any.
 We
are almost there when our driver, Ravi, pulls over. The van has a flat
tire. Out comes most of the luggage (and we
are not
traveling light; with clothing and supplies for the entire
10 day trip, as
well
as toys and art materials). We pile ourselves
and our
luggage
out of the car, and wait while Ravi tries to find the jack
to raise
the car. He finds most of it, missing however the crucial
piece that is the crossbar, with the socket end to remove the nuts
that hold
the tire on. Fortunately, we have stopped in a well-lit place
by the university,
and Ravi is able to borrow the cross piece of the jack.
We stand around swatting at mosquitoes until Nimmi’s father,
Roger, suggests that we put mosquito
repellant. We find later that the mosquitoes
are very resilient in Sri Lanka, finding the tiniest area
of skin not covered with DEET. Poor Valerie awakens one morning with
swollen eyelids; it
had not occurred to her to put the repellant on her eyelids. “DEET
UP” becomes a clarion call of the group, morning and evening.
We
are almost there when our driver, Ravi, pulls over. The van has a flat
tire. Out comes most of the luggage (and we
are not
traveling light; with clothing and supplies for the entire
10 day trip, as
well
as toys and art materials). We pile ourselves
and our
luggage
out of the car, and wait while Ravi tries to find the jack
to raise
the car. He finds most of it, missing however the crucial
piece that is the crossbar, with the socket end to remove the nuts
that hold
the tire on. Fortunately, we have stopped in a well-lit place
by the university,
and Ravi is able to borrow the cross piece of the jack.
We stand around swatting at mosquitoes until Nimmi’s father,
Roger, suggests that we put mosquito
repellant. We find later that the mosquitoes
are very resilient in Sri Lanka, finding the tiniest area
of skin not covered with DEET. Poor Valerie awakens one morning with
swollen eyelids; it
had not occurred to her to put the repellant on her eyelids. “DEET
UP” becomes a clarion call of the group, morning and evening.
We drive further, and are ‘almost there’ when the lights go out
on the van. This is very dangerous, as the road is narrow and the
people drive like maniacs. (It doesn't help my sense of mastery that Sri Lanka
has right hand drive; I keep being surprised by trucks and busses roaring
toward us on the right.) I feel as if I am in one of my son’s
video games, in which driving on a road means taking your life into your hands.
We
find
out later
that traffic fatalities are the leading cause of death in Sri Lanka,
followed by snakebites. We scrounge around in our luggage and find flashlights,
and
Nimmi hold a flashlight through the windshield as Ravi drives.
We are grateful for Ravi’s driving skills, as in the morning
we see that he has successfully navigated between the sea on one side and the
sewer trench
on the other. There are cows and goats to be avoided as well; somehow,
Ravi got us safely to the orphanage. Later we draft Ravi into our team
to work with the children; he knows how to play cricket!

We finally find our destination, St, John’s, an “American Ceylon” mission
that is an orphanage and school for children whose families have
died in the war. The children run out to greet Nimmi, who has visited before. Jeff
Greenwald wrote in his Field
Journals: A Journey Through the EastJanuary
19, 2005:
Jeff
Greenwald wrote in his Field
Journals: A Journey Through the EastJanuary
19, 2005:
"At the St. John’s Tsunami Relief and Rehabilitation
Center in Batticaloa, an Episcopal Reverend known as “Father J” (short
for Jeyanesan) is spearheading a multi-level effort that includes orphanages,
feeding
centers,
vocational training, and emergency relief supplies. (The popular Reverend was
already immersed in refugee work, providing for families displaced by the civil
war, when the Tsunami struck. Trained at the Hebrew University in Jerusalem,
Father J’s commitment to spiritual integration is immediately obvious;
St. John’s is the first church I’ve seen with a Jewish mezuzah
on its doorway.)"
We stumble upstairs to a large airy room and have dinner. This dinner,
to be repeated every night we are here, consists of cold
rice noodles, a sauce of coconut milk with a yellow spice in it, a curry
with
chucks of meat
and
bone, cut up and steamed carrots and green beans. We see
there are no utensils, so we follow Nimmi and Prabha’s
lead as we eat with our hands. One
never touches food with the left hand, ever, as that hand is used for
cleaning oneself. Joe, who is left handed, has to sit on his left hand
in order not to use it. I find that I cannot bring myself to eat any
fish
here, fearing, as the villagers do, that the fish might have eaten the
dead. There are charts in the papers to show what fish feed on, to reassure
us that the fish are safe to eat, but I can't make myself do it.
The
room upstairs is large and airy, and we think it will be a good place
to sleep. We find out, however, that only the men
will sleep
there. The
women go down to beds in the girl’s dormitory, bunk beds.
The girls flock to us, touching, talking in Tamil. They are
very curious about us, and call us “Auntie’,
which is a sign of respect given to an older woman. They
quickly
find
something to tease us about; for Valerie it
is her long nose (which to my Western aesthetic seems
on the short side), for me it is my lack of earrings,
as I
have removed
my earrings due to sore piercings.
They tug at their earrings and then reach for my sore
and inflamed ear lobes. I am determined to find earrings
that
are not as
heavy as the ones I was wearing,
and put antibiotic ointment on my earlobes before bed.
Getting ready for bed is a challenge. The girls are very modest,
and so I take my clothes with me to the shower. What shower?
Bathing take
place
in
a large
red bucket, with a smaller pitcher. You use the pitcher to
pour water over you, then soap down, and rinse again with water from
the pitcher.
There
is no hot water, and by the end of our stay there, I am in
agreement
with the ‘what
do you need hot water for in the tropics anyway?’ school
of thought. Right now, it is a shock, and I just cannot deal
with it.
After the plane trips, the long ride from Colombo, dinner eaten with my
hands, I confess to a moment of Western princessness; I want a real shower
and a room of my own! Not. Instead of braving the shower, the big red bucket,
I use wipes to clean myself, and try to change into sleeping clothes without
getting
them
wet, as
there is water everywhere in the floor. I do a little dance of rolling up
my pants leg, getting my feet in and out of my flip-flops, getting my legs
through the pants, without getting them wet. I am not quite successful,
so spend
the
first night with pants wet around the ankle. At least it is water from the
bath, and not the toilet!


All ready for bed, and I cannot sleep. I wander out and run into Selvie, the
lovely 30-year-old woman who is in charge of all the girls at the orphanage.
Selvie
speaks some English, and we find ourselves sitting on a bench, talking.
She is “amah” or mother to 175 girls! I compliment her,
and say that I an amah to only three children , and I cannot imagine
how she does it. The girls call her  “Selvie-amah”.
I tell her that I will be a grandmother in July, so my name becomes ‘Amahmah”,
or grandmother. Soon all the children call me “Amahmah”. Selvie
and I talk a bit, but every minute
a girl comes up to her for something; she is mother, nurse, soother, everything
to 175 girls. She also supervises the wardens, or young women
who serve as house mothers. They get to go home each night if they have
one, while Selvie-amah lives at the orphanage with the girls.
“Selvie-amah”.
I tell her that I will be a grandmother in July, so my name becomes ‘Amahmah”,
or grandmother. Soon all the children call me “Amahmah”. Selvie
and I talk a bit, but every minute
a girl comes up to her for something; she is mother, nurse, soother, everything
to 175 girls. She also supervises the wardens, or young women
who serve as house mothers. They get to go home each night if they have
one, while Selvie-amah lives at the orphanage with the girls.
Things have
become complicated
lately, as the Tamil Tigers, as a gesture of good will, released
their child soldiers to Unicef. Unicef turned the children over to the
orphanages, the place where they would be safest. Selvie has to integrate
adolescent
girls
who were soldiers into the community of proper Christian-schooled girls.
The child soldiers are the ones with short hair, and they stick together.
The culture
of the army and the culture of the orphanage are quite different, and I
wonder how long, if ever, it will take for the soldiers to blend in with
the cloistered
girls. Finally, I am sleepy enough to try to go to bed; so I find my bunk
in the dormitory and sleep. Our team begins to joke about the the
Southern team; we call them the 'resort humanitarians', because they are
eating in
restaurants and staying in hotels. (We find out later they visited 10 refugee
camps; hardly the 'resort' life we had fantasized for them!) What we lack
in comfort at the orphanage, however, is more than compensated for by the
warmth with which
we are embraced
by
the children and staff at St. John's.

Tuesday
I awake at 4:30 a.m. to the chatter and laughter of girls, the sounds of sweeping
and mopping. Bathing is done by seniority, so if the younger girls want to
bathe, they must
get
up very early to complete their chores before the ‘showers’ are
taken over by the older girls. I try to get back to sleep,
but my body has no idea of the day or the time. We have breakfast, a cold
fried
egg with bread and dried coconut flakes, very spicy and good. We are eating
with our hands, but cold egg defeats us, until we see that Prabha
has made an egg sandwich. We have tiny
bananas that grow in Sri Lanka; if the bananas in the States tasted this
good I would eat them every day. They grow in bunches and are sweet and creamy.
We also meet up with OperationUSA's
water team, who are giving people small hand pumps to filter water from their
wells. Carinne Meyer's report is online at http://www.operationusa.org/sri%20Lanka/field%20report.htm.
We get into the van to go meet the people who have arranged the training.
En route, we see houses damaged, and ask it is from the Tsunami. “No,
it is from the war. Fighting was here; this house was damaged by a
bomb, here
you see bullet holes.” We realize, that, other than flooded rice fields
(a huge concern, as the fields were inundated with salt water and sewage…how
will there be enough rice to feed the people?) we have yet to see Tsunami damage.
We are greeted by Father Paul Satkunayagam, Director and Co-founder of the “Butterfly
Peace Garden”. Children traumatized by the war
can come here to begin healing, and groups are run to
promote understanding and peace. I fall in love with The Butterfly Peace Garden,
and its mission:
The Butterfly Peace Garden is located in the Batticaloa district
of Sri Lanka, a region where many lives and communities have been profoundly
affected by a long-running civil war. For seven years now the Garden has
provided a sanctuary where thousands of children from villages and towns
throughout eastern Sri Lanka have come to play, cultivate the soil, care
for animals, practice arts such as music, painting, sculpture, ceramics,
theatre and learn basic elements of yoga, qigong and other body wisdom
exercises. Most importantly, the Butterfly Peace Garden is a place where
children have the opportunity to simply be kids again. As they make and
mend in the Garden, the children who pass through its gates become healers
in their communities, their nation and their world.
The
Butterfly Peace Garden opened its gates on September 11, 1996, and since
then it has been bringing together artists, peace-workers,
ritual healers and counselors with children from Batticaloa's various ethnic
and religious groups - Tamil, Muslim, Hindu, Christian - in an oasis of
peace amid the devastation of a civil war that has raged for two decades.
The children of the Butterfly Peace Garden are a remarkable tribe of magicians
who provide living testimony of the power of play as a tool in the lost
art of making peace."
(source: http://www.thestupidschool.ca/bpg/index2.html)
"Children
from six to sixteen years of age attend the Butterfly Garden for nine
months, one day a week, in groups of fifty drawn from the
local Tamil and Muslim populations. Many of them have endured profound
family loss and witnessed great horror: they are the children of terror.
In the Butterfly Garden these children are slowly restored to themselves
and to the world through play and storytelling, music and drama, the arts
of painting and puppetry and participation in the life of a garden. Reconstructed
rituals of genogram-making (The Mother-Father Journey) allow them to begin
telling the story of their families and their villages; group storytelling
allows them to find the narrative and dramatic power to represent new worlds
of their own making. Many of the Butterfly Garden staff were themselves
child victims of the war, and working there is for them a process of healing
and recovery. The work of the Butterfly Garden extends to the villages
in the countryside through a program of outreach and by means of the Butterfly
Garden Bus, which was a gift from the World University Services of Canada."(source: Geist
No. 33, 1999
We
are met here by a group of several men, called MEESAN (Modern
Economics Education and Social Affairs Network) who want to hear about what
we intend
to do, and to make sure it is culturally sensitive. Too many Westerners
have come in to work and apparently, they either leave the children a wreck
(we
hear of someone who came to do EMDR with the children, and left them all
sobbing and unglued as she or he caught a flight back to the States) or just
come in and lecture the workers about what the children need. We are
determined to be different. We decide the best use of our time and talents
is to ‘train
the trainers’, and so a group of 18 people who work with children
are invited to come to our trainings. David explains the exercises and
play activities
to the group.

The men also review our exercises, cognitive behavioral puppet shows and
games that are geared toward mastery of trauma, and agree that they
will not disrupt
the culture. Where we are, in the East, most of the children are Hindu or
Muslim. The team in the South is dealing with Buddhist children.
Each
team finds quickly that we need to modify certain elements of our games.
That afternoon we meet with the trainers to find out their needs, teach
them our techniques, and get to know each other. I become the designated
icebreaker,
and while the rest of the team sets up, I offer each person a cinnamon Altoids,
and then go around and put a butterfly sticker on each person's hand. I make
eye contact when I do, and see incredible wisdom and pain in their
eyes. They are called “animators” (no one seemed to know
why) and they work with the children. Until the Tsunami, their role
was to help the children
with war trauma.
As I hand out the stickers, they tell me that a butterfly is called “Vannathupoochi” in
Tamil, and I try to say it to each person. When I get toward the end of
the group, someone started singing a song about “Vannathupoochi” in
Tamil, which amazingly, goes to the tune of “Frère Jacques”.
I try to sing along, bringing gales of laughter from the people. This song
becomes my theme, and somehow, by osmosis, the children at the orphanage
start singing it to me as well. It is perfect, and when I tell the trainers
how the
butterfly motif has appeared spontaneously in the psyches of children with
whom I have worked that are facing death, they nod in agreement. I tell
them of the children in the concentration camps
who had
carved butterflies with their fingernails in the wood, and again they nod
"yes". They know firsthand the grave loss and despair that seems to summon
the butterfly.
Sri Lankan nodding “yes” is like that of a dancer; somehow, the
head goes back and forth, and the neck moves sideways. When I try it, I feel
like I do when I try to show children how an owl can look backwards; my neck
muscles cannot do this at all! More gales of laughter when we try to nod ‘yes’ to
the trainers. This learning to nod becomes David’s theme with the trainers;
they tease him as he good humoredly tried to do it. We learn there is a subtle
difference between nodding ‘yes’ and ‘I don’t know” and “no”;
I think I would have to stay for years to understand the nodding, much less
master it.
The men and women animators are amazing; they have such a depth of compassion
for the children. We start by asking them what they want from us. They are
exhausted, and need some new ideas, specific to the Tsunami. We learn later
that two of the women who are working with the children are also refugees;
they have lost everything, and are living in tents side by side with the
children. We realize that these workers are suffering from ‘compassion
fatigue’,
so part of our plan is to help them refuel, to play with them, and give them
an opportunity to tell us what it is like for them. We know, however, not
to push, but to hold the space so that if they feel safe enough, they may
tell
us what they are going through. I am in awe of these animators, who have
been on the front lines of trauma for years: first the war, and now the Tsunami;
yet still, they smile. One of the animators, Shanty, shows us a drawing and
story by a girl who was rescued by a helicopter; she was in the water from
the
time
of the
Tsunami
at 8:00 a.m. to her rescue after 3:00 p.m. Her story shows the progression
from the trauma to the rescue, showing great resilience.
Shanty
tells us the
girl
is
only
11 years old; she is living in the refugee camp now.
I ask the man sitting near me if he could please translate, as our Tamil
speakers are elsewhere. He graciously agrees, and I find out later
(with embarrassment!) he is Mr. Sornalingam,
of the Sri Lanka Centre for Development Facilitation (SLCDF), and a very
important man. Again and again, I see great humility
in the people here, and incredible beauty.
I can
hardly imagine what their lives must be like - 20 years of civil war, and
now the Tsunami. One woman said it so eloquently to Prabha, “We
lost so many in 20 years of fighting, and then we lost more in 20 minutes
of the Tsunami.” I
have such respect for these trainers, and know that they will teach me more
than I could possibly teach them. They have been to hell and back, and
survived, still their faces shine, and they smile through tear-filled eyes.
We adapt some of our exercises based upon their feedback; “Go fish” becomes “Go
choose” until we realize that card games of any type are taboo, due
to the association with gambling. Our game of "fishing”; using
a pole with a magnet on it to pick up a felt fish with a coping method written
on
it, becomes instead "bobbing for apples". We don’t
want the fish aspect to be a ‘trauma trigger’ but instead want
the children to concentrate on the coping methods. “Stone soup” becomes “Tsunami
Samba”, samba being a type of stew.
We
then drive to the beach to see the damage first hand. We are shocked, speechless,
horrified. There are no words.


We are stunned into silence. The devastation is immense. Cement foundations
are cracked, walls torn off houses and temples. One beautiful Hindu temple
was halved; we speak to the priest, who was inside praying at the time
of the Tsunami. He was safe in the inner sanctum of the temple; it is
considered a
miracle. The back of the temple is torn off, the front still intact.


We
see a beach that was covered with fishing shacks; this beach looks
empty, there is no sign that any homes had once been there. But on the beach
where we are now, there were hotels, and houses made of cement and stone.
All is demolished. Coconut trees are downed. Some of the trees have saris
still caught in them. These are the saddest, because these trees had women
clinging to them, women who were then torn out of their clothes, out of the
trees, to their deaths. We see an occasional shoe, a flip-flop, a
dress in the debris.

A few
people are working, trying to remove debris from where their homes were.
They are carrying away broken boards, bricks and chunks of cement by
hand, and in baskets.
There is no sign of any heavy equipment.

In
the East, Tamil country, people believe that all the resources are going
to the South, to the Singhalese.
We hear later, from our Southern team, that the people in the
South believed all
of the help
is going to the East. We wonder where the billions of dollars of
aid are going; certainly not to clearing the beaches of rubble, should people
decide to rebuild.
This is more than one month after the Tsunami, yet very little clean-up
appears to have
been done. We see white flags
of mourning, and a grave, or memorial marker, surrounded by red flags.
So much is lost.

People are also disturbed by a plan in which they must go 1,000 km inland to
rebuild, yet the hotels can rebuild on the beach. It seems so unfair
to the people; in this land of bicycles, how would a fisherman get to his
boat? Get his catch home? Yet many are also unsure if they ever want
to see the sea
again. How could you ever feel safe again in a place that has destroyed your
family, decimated your home? No one believes he or she would ever sleep through
the night living by the sea, yet no one wants to be forced to move.
We hear from people that after the Tsunami, there were hundreds
of bodies on this beach. It is impossible to imagine such devastation looking
at the sea today, which is calm and brilliantly blue.
We
hear that snakes caused the Tsunami. In fact, two days before the Tsunami,
blue water snakes
curled
around a nearby bridge. People were frightened, and believed that it
meant war was returning. Later speculation was that the snakes somehow sensed
the
heat generated
by the ensuing earthquake, so fled to the bridge. We drive over that
bridge;
the snakes are gone now.
We heard repeatedly of the animals; that shortly before the Tsunami
hit, the animals all fled to higher ground. Many people died, while few
of the animals
did. Reuters reported on December 29, 2004, "The strange thing is
we haven't recorded any dead animals," H.D.
Ratnayake, deputy director of the national Wildlife Department, told Reuters
on Wednesday. "No elephants are dead, not even a dead hare or rabbit," he added. "I
think animals can sense disaster. They have a sixth sense. They know when
things are happening."
Another story was that a statue of the Buddha floated over from
Thailand, and caused the Tsunami upon hitting the Sri Lankan shore. We heard
of two temples to different deities that were too close together; the gods
of these temples warred, and caused the Tsunami. We hear that UFOs
were sighted before the Tsunami hit. Another rumor swirling
around was that underground
nuclear testing that caused the Tsunami.
Walking on the beach, we see few people. Those that are there look absolutely
haunted. The ones who want to talk come up to us and tell their stories.
Through translation, we hear again and again stories of death and destruction. “The
first wave took my house, the second wave my children, and the third wave
my wife. What do I have to live for?” “My baby was ripped
out of my arms.” We are near Kalmunai, where the famous "Baby
81"; the eighty-first person admitted to the hospital, was found.
So far, eight heartbroken and desperate couples have claimed this baby
as their lost child. “I
lost my 5 year old son, my 10 year old son.” “Lost, lost, all
is lost.”
We are sobered, going back to the orphanage. Here the children talk with
us, some are studying English. They all want us to know their names and ages.
One
girl tells me about the “bomb” that killed her mother, her father,
and her brother during the war. The little house was left for her was
destroyed during the Tsunami. "Bomb" and "Gone" are her
English words. The
children are full of sorrow and joy, reflecting both in their wise eyes.
They have lived through things we in America have no inkling of; civil war
and then
the Tsunami. I am grateful for the orphanages, knowing the huge amount
of child
trafficking and prostitution that occurs to orphans. My heart breaks again
and again.
The girls see my butterfly sticker, and repeat “Vannathupoochi”.
I hum a few bars of ‘Frère Jacques’ and the girls sing the
butterfly song to the same tune. They try to teach me the words, giggling at
my Tamil pronunciation. Later, every time they see me, they call out, “Amahmah,
Grandma, Vannathupoochi” and start to sing the sound, with accompanying
arms gestures as butterfly wings.
Vannat-hu-poo-chi
Vannat-hu-poo-chi
Parakkuthu
Par
Parakkuthu Par
Ailagana
Chettai
Ailagana Chettai
Adikkuthu Par
Adikkuthu Par
(very
rough translation...if anyone knows the correct spelling and meaning, please
e-mail me!
Here's the tune, courtesy of
Mickey Gentle at Laura's Midi Heaven)
Butterfly
Butterfly
Wings
we see
Wings we see
Beautiful Wings
Beautiful Wings
See the flight
See the flight

We have dinner, and the team talks about the day, what worked, what didn't,
what we want to do tomorrow. We share our sadness and shock about being on
the beach, when the full horror of the Tsunami hit us. Daily debriefing
became very
important
to us,
as
we needed
to help each other deal with the torrent of loss and pain we were facing
and feeling. The name for this phenomenon is “vicarious traumatization”;
it describes how a person can feel holding so much of another’s pain.
We needed each other, and the laughter of the children at the orphanage helped
as well.
That
night I braved the shower. Sri Lanka is very humid, and I felt so sweaty
and sticky that the idea of dumping a pitcher of water over my head
was quite appealing.
Bracing myself, I poured
cold
water over my head, then I soaped down and rinsed off. It
felt wonderful! My hair was
more problematic, as it hangs to my waist and tends to snarl. Finally,
in order to rinse out the shampoo, I just stuck
my head under the faucet. I had to be careful not to take even a sip of the
water. As it would have been scandalous to go upstairs to the
open
room, with
its cool breezes, because
the men were there, I had to stay in the girl’s dorm (hot, airless,
humid...AAARGH!)to untangle my hair. I also resisted the girl’s attempts
to help brush and fix my hair, as I did not want to get head lice. I used ‘tea
tree oil’ to ward off the lice, so I smelled somewhat like a tree.
Any mention of lice would start my scalp itching like crazy. In fact, if
someone
had offered me an opportunity to go to Sri Lanka, to a
land of malaria-bearing mosquitoes, snakes, head lice, humidity,
showers
that were buckets of cold water, unmentionable toilets, winding, dangerous
roads, I would have said they were insane. I would have declined, even if
they had
paid
me to
go. Yet here I was, volunteering, having paid my own way, and truly loving
it.
Go figure…I think it is the people who made the difference, as they
are so warm and wonderful, and perhaps the hope that I could help even a
little bit.
It was quite late after my hair was finally unsnarled and properly braided
by Prabha, so I went out and found my friend, the housemother, Selvie-amah.
She
has
such a gentle
way about her. As we talked, she told me she had lost two of her brothers
in the war. I asked her how she takes care of herself. It seemed a hard
concept
for her,
and for many of the workers I met. Taking care of
oneself was an alien idea. Here, when I work with people, I use the metaphor
of what
flight attendants say when they are going over the safety features on
the airlines, “In the event of an emergency, if the oxygen masks come
down, and you are sitting with a child or someone who is incapable of taking
care
of themselves, put YOUR mask on first, then take care of them."
This image
would not work in Sri Lanka, because most people had not been on an airplane.
Not
only was my metaphor a dud, but the whole idea of taking care of oneself
seemed self-centered, against the grain of the culture. Finally, Selvie-amah
told
me that she loves to listen to Christian music, and starts and ends each
day with that. I laughed, telling her of my Sunday morning ritual of listening
to
KDFC’s (San Francisco’s classical music station) Sacred Music
concert on the radio, in spite of my husband and son moaning about
it.
I go
to bed, wishing I had known our lodging arrangements prior to leaving home,
as mosquito netting would have made a huge difference in my comfort level.
I
tried
to read a bit
in bed, but soon fall asleep. I was a bit nervous that my childhood and
young adulthood nightmare of a huge wave, black with fury, would recur in
the land
where the Tsunami had hit, but it did not. I was surprised, though,
at how much my dream Tsunami matched that of the survivors' descriptions.
I never knew consciously that tidal waves were black, yet my nightmare
wave always was. Again and again we heard of the
big black wave that took everything.
Wednesday
After our egg breakfast, we go to a new space, the Mangrove Center, to
continue to train the trainers. It is raining outside, and we cannot
turn on the fan, due to a leak in the roof, water was in the
fan motor. Every person
who joins us late starts to turn on the fan, and we yell out "No!",
acting out an electric shock. The room is very hot and humid; sweat is pouring
off me,
which I hate. Once again, I open with the cinnamon Altoids, the butterfly
stickers, and the “Vannathupoochi” song. This
time, because the team is not quite ready, I go around again with flower
stickers. They teach me the
word for flower is “poo”, and I try to repeat the colors. Everyone
is laughing by the time the team is ready. Our translator is Anita Nesiah,
a brilliant woman with two master's degrees, and a Ph.D., who taught at Harvard
when she lived in the States. Prabha, speaking Tam il
with Anita, teaches the puppet show to the trainers. Prabha is so full of
life and energy - everyone
loves her. I wish I could speak Tamil, as she does, to not to have to rely
on a
translator.
il
with Anita, teaches the puppet show to the trainers. Prabha is so full of
life and energy - everyone
loves her. I wish I could speak Tamil, as she does, to not to have to rely
on a
translator.
We teach the animators our games and exercises, and then, when the rain clears,
go outside to show them a version of "Follow the Leader”.
This is Valerie’s
contribution, and she is wonderful - very animated and joyful. She includes
some yoga. My favorite exercise is when she has us “reach for the
stars” grab
them, then, “Whoosh” bring them down to earth. She is the
leader in "Follow the Leader”, and then, having learned the the Tamil word
for leader, points to someone else in the group, designating him or her
as the
leader,
and
we all
follow.
Soon we are jumping, hopping, and laughing.

An
older woman wanders in to the yard in which we are playing. Two young
girls accompany her. We
invite
them all
to join
us. They
do,
and then suddenly
the woman starts sobbing and keening. I go over to her, and I
hold her and rub her back as sobs pour out of her. She wails with pain,
her cries almost
a song. She somehow communicates to me that she has lost 41 members
if her family in the Tsunami. 41! I cannot even begin to imagine her pain.
A world
of pain. Sometimes there is nothing to do except hold someone, rock
with
them in their pain. Show up. Be as human, and humble as you can, because
you certainly cannot fix it, or heal it, or make it go away, or even comprehend
this level of loss. She gestures, and somehow I know she has lost children
and
grandchildren. She
makes a slashing
gesture
around
her
neck,
and I am
concerned
that
she
is suicidal. Sri Lanka has one of the highest suicide rates in
the world,
and I am very worried about this woman. I call Anita over,
and describing the woman’s gesture, ask her to find out what
it means. Anita listens for a while, and tells me the woman is referring
to her
husband,
to the necklaces she wore when she was married. She was gesturing that
she had lost her husband in the Tsunami, not that she was suicidal. She
had been in the hospital
when the Tsunami hit, killing most of her family. The two little girls
with her are the two grandchildren who survived, and they look like they
are in
shock. One of our workers plays with them as I try to console the woman;
knowing that consolation is impossible. So I witness her pain, rocking
with her. When
she looks into my eyes, she sees my tears, mutely reflecting her
excruciating
pain. The little girls keep looking at their grandmother, not knowing
what to do. They look very scared, they too have lost almost everything
and everybody. One of the trainers comes up and agrees to help the grandmother
find the resources she needs. My heart breaks; this woman's unbearable
loss stays with me.
We finish the morning training session, have a quick lunch in town, and then
head to a refugee camp.
This camp, Valaichenai,
is
housed
at
the Pentecostal Church, Karuwakerni mission building; it
is a huge open two-story building. Shanty and her
co-workers, Thaya and Mansulla greet us. Shanty takes me inside and shows
me a young boy who is lying on a mat. She explains
that
he has
lost
his
two brothers,
one age 5, one age 10. His mother sits up, looking at us with tear-rimmed
eyes. His father is also lying down. Shanty says the boy hardly moves,
ever. She
is very worried about him. Looking at him, I realize that my project for
the day, drawing, should be done in the shelter, because children like
this boy
will not come to another space.
Our
team decides who will do what;
Prabha and David will do the puppet show, and Valerie (with Ravi's help)
will do active, outdoor activities, like cricket, volleyball,
and
follow the leader, while Joe will make “support necklaces”.
In this activity, a child makes a necklace out of colorful pieces of foam,
putting on the foam the names of people they can count on to be there for
them. Joe has a very calm manner, and the children flock to him. I
will do art, hoping to do a sequence of drawings with the children (and
maybe
some
parents,
who
knows?)
in which
they can
draw
whatever
they want. If they draw the Tsunami, my task is to lead them through
a series of questions, “What happened next?” to the realization
of where they are now, and that they were relatively safe. It is very hard
to do
trauma work in a refugee camp, because of the hierarchy of needs; food
and shelter
come before anything else. Yet play and drawing are the first languages
of children, and we could see how depressed the children and adults were.
It
was eerily silent; later we learned there were hundreds of children
in the camp, with no toys, no supplies,
nothing. And this is more than one month after the Tsunami. Government
reports of
January 11 state there were 416 families, a
total of 1,263 people, housed in this camp alone.

I go to get the art supplies, generously donated by some of my local schools:
The Mountain School, Good Shepherd School, and Novato Charter School.
They have also given me letters and drawings from the children, ranging from
poignant ones from kindergartners, who did water colors, and said,
"We love
you", to those from the seventh graders, who did beautiful drawings. I
wanted the children in Sri Lanka to know that there were children from
far away
who cared about them.
Trudging
across a field to get the art materials, I see that the camp leaders
have brought a huge group of children to
an
area to see the puppet show. But, alas, no David and Prabha, as
they are furiously
working to get the dialogue translated into Tamil. The children are starting
to fidget and fight. I went to them, and asked someone to translate
for me. I
tell them there once was a caterpillar. Then I asked what happens to caterpillars,
and the children answered ‘cocoon’ (I am not even going to
try that in Tamil!). “And then what happens?” I asked. “Vannathupoochi” and
so began a round of “Vannathupoochi”, sung to
the tune of Frère Jacques. I kept looking for the puppeteers to
appear, abut no such luck! Some of the children came to the front of the
group and sang
solos,
ending when one tiny child came to the front.( She was the size of an American
three year old, but probably was about seven years old. We were invariably
wrong
when we tried
to estimate
children’s ages, off by years. Whether it was child nutrition,
or genetics, the people of Sri Lanka are much smaller than Americans. Sometimes,
at 5’3”, I felt like a giant.) She sang “Vannathupoochi” beautifully,
then segued into “Frère Jacques”, ending with the English
version, “Brother John”.
Still no puppeteers, so the children and I made up a story. I asked the children
what “Vannathupoochi” did. “He
flew” they answered, so we all flapped our wings. “And what
did he see?” and
the children yelled out various things, until their voices were drowned
out by the sound of a train. The workers tried in vain to get the children
to stay
seated, but of course, they wanted to see the train. Knowing from years
of experience that to resist is sometimes fruitless, in the story, Vannathupoochi
sees a train. The train came and went; the trees mostly hid it.
One
child
quipped that “Vannathupoochi” did not see the train,
and everyone laughed. The story continued with “Vannathupoochi” hearing
the train, and continuing his journey. Finally, the puppet crew came, so
the butterfly landed on a flower and I said good-bye. I grabbed art supplies
and headed to the shelter.
My
goal was simple: to try to engage some of the children and parents in an
art/play activity. The lethargy in the camp was palpable; many children and
adults just lay on mats, depressed. People were surrounded by their belongings;
pitifully small amounts that they were able to salvage, or had been given
to them. I imagine for a minute if everything I had was lost; if all I had
were a few items of donated clothing, maybe a few mats on which to put on
the concrete floor. Yet, that would pale if I had lost my family. I keep
remembering the woman at the Mangrove Center who had lost 41 members of
her family. How do you go on after that?
I went
to a clear space on the floor and started to sit down. Before I knew it,
mats were appearing. I sat on a mat and put  out
some brightly colored paper, markers, and crayons, thinking perhaps a few
children would come, and then
maybe I could engage their parents. Within minutes, children and
adults surrounded me. I was handing out paper and crayons like mad. This
was not going to be a small group exercise, leading people through the "what
happened next?" scenario; this was free-form chaos. Adults as well as
children wanted to draw, mostly pictures of the Tsunami. I gave
no
direction, they sat and drew, and drew. Children and adults approached,
showing me their drawings. Almost everyone wanted their picture taken with
their drawing.
out
some brightly colored paper, markers, and crayons, thinking perhaps a few
children would come, and then
maybe I could engage their parents. Within minutes, children and
adults surrounded me. I was handing out paper and crayons like mad. This
was not going to be a small group exercise, leading people through the "what
happened next?" scenario; this was free-form chaos. Adults as well as
children wanted to draw, mostly pictures of the Tsunami. I gave
no
direction, they sat and drew, and drew. Children and adults approached,
showing me their drawings. Almost everyone wanted their picture taken with
their drawing.

Once
people were settled into drawing, I walked around the shelter, giving out
paper and crayons to the ones who had not come forward. These were the people
I was most concerned about, the children and adults so overcome with depression
that they lay on their mats on the concrete floor. The first family group
I gave art supplies to is that of the little boy who Shanty had pointed out,
the one who hardly moved. I wandered through the camp, handing out markers,
crayons, and paper. There are
so many
children here! I could only give a few crayons to each child; I wished
for the abundance of being able to give each child a whole pack of crayons,
so
that
he or
she could have all the colors from which to choose.
Returning
to the main group, I see the drawings range from depictions of the Tsunami
to lotuses and doves. Some of the people have included a chronology in the
drawings; you can see a whole sequence of events portrayed. These people had
discovered the "what happens next?" technique on their own.





 It
is hard to say good-bye to the children. Joe shows the children their images
from the back of his digital camera; like all children, they love to see
themselves.
It
is hard to say good-bye to the children. Joe shows the children their images
from the back of his digital camera; like all children, they love to see
themselves.
I think
we are all feeling inadequate to the task, overwhelmed
by the numbers of children and adults. I wish I could have a year just to
work with the people at this one shelter.
As
we leave, I am pleased to see the boy who had been lying on his mat, so depressed,
had
joined
the circle of children drawing.

After
our visit to the camp, our translator, Anita,
suggests that we go to the beach in Batticaloa where the people we had just
seen in the shelter had lived. She tells us she used to go a hotel there;
all is gone. Nothing is left. Again, it is seeing the
saris caught on the ruins and in the trees that make my heart clutch. Were
women torn out of them by the Tsunami?

Thursday
Again,
we are up and out the door. I am finding it difficult to have so
little time and solitude. I have not been alone since boarding the Airporter
bus in San Francisco. Technology is defeating me; it is difficult to use
the
laptop to write, and
downloading
photographs
is
impossible.
In Batticaloa, there are intermittent power outages, and the
system to charge a battery-operated device, such as a camera or laptop, takes
all of Joe's knowledge and wizardry. My adaptors and transformers don't
work at all.
Thursday
morning we return to the Butterfly Peace Garden to meet with the trainers,
and again
I greet
them
with cinnamon Altoids, butterfly and flower
stickers, and the now famous (or infamous) butterfly song. Valerie has
threatened me with death, because she can't get the butterfly song out of
her head.
When one of the
workers comments that I am a "little crazy" about butterflies,
I laugh, and agree. How do I explain the synchronicity of the stickers,
the song, the butterfly peace garden? I think butterflies picked us, we did
not choose them.
We
again start the session asking the animators what they need, and, after teaching
a few more
protocols,
they
begin
to speak
of their
experiences.
Shanty tells us her sister lost both of her children in the Tsunami.
Fajriya and Rifaya are refugees, living in the camp in which they work. Everyone
speaks
of
loss,
of burnout.
They have
no more creative energy to come up with ideas - every cell in their
bodies is saturated with pain and trauma; they are exhausted. We hold
them as a group; hoping our containment and caring can at least let them
know
that we care. It would be arrogant to say that 'we know', because, how
could we? Our group has developed such respect for these workers, and
such humility. As
always, they have taught us much more than we have taught them; given
us more than they have given us. They humble us.
Thursday afternoon, the group returns to the Butterfly Peace Garden.
Learning from the chaos of our visit to the camp, and the difficulty
of working
with so many children at once, has led us to the idea of creating 'stations';
Joe, Prabha, Valerie
and David each take an activity, and working with one of the Sri Lankan
trainers, play with a group of children. The children rotate through
the stations, so, instead of all the children doing an activity at once,
only
a quarter of them do.
I stay
back at the orphanage to do an exercise with the younger children. As we
call them, more and more children come, so at the end there seem to be over
100
young children. Their housemothers help me, and we make “Vannathupoochis”, folding
a piece of paper in half, and drawing one side of a butterfly on the paper.
Cutting it out, when you open the paper, there is a full
butterfly. The children then use crayons and stickers to decorate the butterflies.
They are beautiful; each child wants me to admire her “Vannathupoochi”.
folding
a piece of paper in half, and drawing one side of a butterfly on the paper.
Cutting it out, when you open the paper, there is a full
butterfly. The children then use crayons and stickers to decorate the butterflies.
They are beautiful; each child wants me to admire her “Vannathupoochi”.

We
end by singing the Butterfly song
.
That
evening, our last night at the orphanage, the children
have arranged a dance for us. Dancing barefoot
is
the best
compassion fatigue exercise in which I have ever participated. Some
of the animators we have been training came to the dance. I inadvertently
ended up having a showdown with one of the girls released by the
Tamil
Tigers.
She
came up
to me
and
started
dancing.
Reminiscent of "West Side Story"; the dance got more
and more aggressive as we postured and imitated each other. I was
so hot I had to
leave
midway
to dump cold water on my head. When I returned, the dance floor
cleared, as the two of us danced. The women were cheering us
on. As the
music ended, I bumped out my hip and her
headband
went
flying. Everyone clapped. I was deemed the winner, but I think
it might have been a tie, because she didn't need to leave to cool
down.
(Hot
flashes
in the tropics are a drag!) By the end of the evening, we were
all glowing with sweat
and joy.

Friday
This
was our
last morning at the orphanage and camps before we began the long journey
home. None of us wanted to leave; we wanted to go North
to Jaffna, to work with the people there. Saying good-bye to the children
and staff at the orphanage was very difficult; I know I was sad to leave,
in spite of mosquitoes, showers from a bucket, hand-washing laundry in a
pail, head lice, the unspeakable toilets, and the 4:30 a.m. wake-up. The
people were so warm and gracious; they will stay in my heart.

We
went back to the Butterfly Peace Garden for a good-bye session and feedback
from
the
trainers. They most appreciated our playfulness; that we, as adults,
would play with them, and with the children. They said they were now playing
more. Saying good-bye to these dedicated workers was very difficult. We then
went
to a
Muslim camp,
Firthous
Refugee
Camp,
Kattankudy. We are greeted by Fajriya and Rifaya and people from Meesan.
Conditions were dismal there; people were living in tents with no floors.
I heard later that the temperature inside the tents could reach 110°.


 We
began to hear reports that many elders perished in the Tsunami;
that the most vulnerable, the children and the elders, were the least able
to
escape the devastation. In fact, we see only a few older people at the refugee
camps.
We
began to hear reports that many elders perished in the Tsunami;
that the most vulnerable, the children and the elders, were the least able
to
escape the devastation. In fact, we see only a few older people at the refugee
camps.
We
have only a little time here, so we go to the classroom to meet the children.
Here we find out that the children are school-aversive; an unusual thing
in Sri Lankan society. The children are very dedicated to school;
literacy rates
are extremely high,
education is seen as the only way out of poverty. Generally the children
wake up early  to
do chores and study, then go to school, then have an hour for chores
and play time.
At 4:30 homework starts. (I am going to try this schedule with my son
when I get home...right!) We are amazed at how well behaved the children
are - they listen to the adults, they sit quietly, and are so well socialized
that I agree when Joe says, "Actually, we could learn a lot about how to
raise children from the people here."
to
do chores and study, then go to school, then have an hour for chores
and play time.
At 4:30 homework starts. (I am going to try this schedule with my son
when I get home...right!) We are amazed at how well behaved the children
are - they listen to the adults, they sit quietly, and are so well socialized
that I agree when Joe says, "Actually, we could learn a lot about how to
raise children from the people here."
The children in the camp are avoiding school; we
don't
know
if it is that they
are reluctant
to leave
their parents
(or
are
the parents reluctant to have their surviving children out of their sight?)
or is it because the school faces the sea? I know that if I had sustained
the losses these people had, I would never let go of my surviving children,
never let them out of my sight. At first the children appear
very serious and sad; as we leave they are smiling. We
have given them letters and drawings done by children from all over the world,
and,
or course, stickers.
They sing “Vannathupoochi” with
me, singing more verses than I ever imagined existed. Valerie did her
magic with "Follow the Leader", and David, as our leader, was
honored by having his hands painted with henna. The woman who did the
henna never
once touched
his hand; indeed, men surrounded her as she worked to make sure that
did not happen.

After
we saw the children we walked on the beach, this time with the people who
had lost their homes. Children would come up to me and say, pointing
to a pile of rubble, "This is my house." My broken heart
surely broke a million more times that day. We reluctantly said good-bye
to begin
the long journey home.



Re-entry
Re-entry
is hard! I nearly burst into tears at the grocery store,
overwhelmed in the shampoo section by how many types and brands
there are.
I want to pack off everything in the store and send it to Sri Lanka,
to the people in the camps and the children in the orphanages.
I am not sleeping very well; I do not think it is jet lag, but
rather
"soul lag". I wake up in the middle of the night and
start to write. How can I be here when so much
of my heart is there?
I keep
thinking, "What next?" What can we, as humans, do, for other humans
who are suffering? I don't know the answer, other than the feeling
that we, who have so much, are not doing enough for those who have
lost everything.
It is
still the eyes that haunt me; the eyes of the woman who lost 41
people in her family, of her two shell-shocked granddaughters,
of the mother whose children were swept away, of the man whose
wife
and children's bodies have not been found. It is the eyes of
the listless children at the refugee camps, and the eyes of the
children who sadly point out where they used to live. My heart
goes out to these people, who have seen war, and death and destruction.
I see pain, shock,
and loss on the faces of the survivors - everything
can change in a nanosecond. Life is fragile and precious. How
do you go on when your village, your home, your family, is destroyed?
I see the faces of those who I met in the refugee
camps, and it is the eyes that capture me. And it is the eyes of
the children that haunt me, and make me unable to sleep through
the night.
Tsunami Journal - A visit to Sri Lanka by Kate Amatruda, LMFT, CST-T, BCETS

Thank
you!
|
My heart
is touched forever ~ thank you for letting me share my journey with
you. Thank you to my wonderful team: Joe, Prabha, Jodi,
Sharolyn, David, Valerie, and Maria, and to Janine Shelby,
Bill Burns and the crew at APT, and everyone at OperationUSA: Nimmi,
Carinne, Ravi, Anita and Skip. Thank you to everyone who donated
to the Foundation at APT. Thank you to
Barbara Amatruda for your kind donation, to the Novato Charter
School, especially
to George Bevins' 7th grade class and to principal Rachel Bishop,
to the Mountain School and Good Shepherd School for sending supplies
and your artwork to the children of Sri Lanka. Thank you Catherine
Craig, for balloons, paper and crayons. Thank you Kevan Rosenberg
for sharing your bar mitzvah money,
and to your mom, Karen, for her last minute run to Costco. Thank
you, Anne at Mrs. Grossman's for the stickers, and CuradUSA for overnight
shipping
two cases
of Clifford Band-Aids, and to everyone else who contributed to
this journey. I feel as if
I took
the spirit
of
my friend, the late Mary Murray, with me. Thank you Kim for running
www.psychceu.com and always to Roy and Colety for all of your love
and support, and to the kittens for getting on the
phone the few times I could manage to call home. Most certainly and
most
especially my eternal gratitude to all the wonderful
children
and adults
of Sri Lanka who opened their hearts to me.
 With
gratitude and love,
With
gratitude and love,
Kate
Kate Amatruda,
LMFT, CST-T, BCETS
45 Hillside Terrace
Novato CA 94945
February
14, 2005
 Kate
Amatruda, LMFT, CST-T, BCETS, is
a Licensed Marriage and Family Therapist, Board Certified
Expert in Traumatic Stress - Diplomat, American Academy
of Experts in Traumatic Stress, and a teaching member
of the International Society for Sandplay Therapy.
She is a Disaster Service Mental Health volunteer with
the Red Cross, and has responded to the Hurricane Katrina
disaster, as well as to local fires and floods with
the Disaster Action Team. She went to Sri Lanka with
the Association for Play Therapy and OperationUSA.
She has lectured internationally and teaches in the
Extended Education departments at U.C. Berkeley and
Sonoma State University. She is the author of A
Field Guide to Disaster Mental Health: Providing Psychological
First Aid, HIV: The Storm, Psyche & Soma, Trauma,
Terror and Treatment, and Painted Ponies: Bipolar
Disorder in Children, Adolescents and Adults. Her
work with trauma is featured in the DVD Trauma Treatment
- September 11 - One Year Later, an hour interview
with Frontiers.TV in Brooklyn, NY, and her work with
children with cancer is shown in the DVD Sandplay
Therapy and the Liminal World. She is the co-author
of Sandplay, The Sacred Healing: A Guide to Symbolic
Process, Reweaving the Web: The Treatment of
Substance Abuse, The Safe Harbor Ethics Series and The
Witch and The Queen. She practices in Northern
California. Kate
Amatruda, LMFT, CST-T, BCETS, is
a Licensed Marriage and Family Therapist, Board Certified
Expert in Traumatic Stress - Diplomat, American Academy
of Experts in Traumatic Stress, and a teaching member
of the International Society for Sandplay Therapy.
She is a Disaster Service Mental Health volunteer with
the Red Cross, and has responded to the Hurricane Katrina
disaster, as well as to local fires and floods with
the Disaster Action Team. She went to Sri Lanka with
the Association for Play Therapy and OperationUSA.
She has lectured internationally and teaches in the
Extended Education departments at U.C. Berkeley and
Sonoma State University. She is the author of A
Field Guide to Disaster Mental Health: Providing Psychological
First Aid, HIV: The Storm, Psyche & Soma, Trauma,
Terror and Treatment, and Painted Ponies: Bipolar
Disorder in Children, Adolescents and Adults. Her
work with trauma is featured in the DVD Trauma Treatment
- September 11 - One Year Later, an hour interview
with Frontiers.TV in Brooklyn, NY, and her work with
children with cancer is shown in the DVD Sandplay
Therapy and the Liminal World. She is the co-author
of Sandplay, The Sacred Healing: A Guide to Symbolic
Process, Reweaving the Web: The Treatment of
Substance Abuse, The Safe Harbor Ethics Series and The
Witch and The Queen. She practices in Northern
California.
|
Webpage,
photographs and contents copyright ©2005-2010 by Kate Amatruda.
All Rights Reserved. All photographs taken with the express permission
of the subject, or subject's parent or guardian (except for the
elephants...)
e-mail:info@psychceu.com