|
|
|
PTSD in Children and Adults Treatment for post-traumatic stress disorder, including assessment, sandplay, play therapy, and verbal therapy techniques, psychopharmacology, and strategies for therapist self-care by
|
Jennifer, age 8
1. Immediately After the Traumatic Event
Sometimes if we can take immediate action there is a subsequent lessening of the emotional toll. The first thing to do is assure the physical safety of the individual.
"Immediate action is important in lessening the effects of traumatic stress," says Valley Trauma Center Executive Director, Patti Dengler. "Most people who are exposed to a traumatic, stressful event experience some of the symptoms of in the days and weeks following exposure. These symptoms generally decrease over time and eventually disappear. However, about 8% of men and 20% of women go on to develop post traumatic stress disorder, and roughly 30% of these individuals develop a chronic form that persists throughout their lifetimes. By working together as a community, we can promote healing in the wake of this shared disaster." (Valley Trauma Center 7116 Sophia Avenue Van Nuys, California 91406)
The second most important thing is to be as present as you can. Avoid platitudes and false reassurances. A wise minister once said, to a parent after the death of a child, "Did anyone tell you that God needed Maria more that you did?" When the parent nodded yes, the minister continued, "I know I could not worship a God that stole my child from me. Such a God would be cruel, and evil." Avoid saying something as simple as, "I know." You don't.
Show up, and don't try to make things better, as you probably can't. Just be there to listen if the person is ready to talk, to just sit nearby if they are not. Sometimes talking is the last thing a person wants to do. It can be reassuring to tell them you know what happened. Kaspar Kiepenheuer wrote of the importance of being present in dealing with children with cancer:
Initially, I suffered from my helplessness in dealing with these children when I believed I ought to do something; and from my speechlessness when I thought it necessary to say something. It was only later that I learned from the children themselves that what mattered was quite different: that is, to be there, to listen and follow them emotionally. This seemed to be a hard thing to do, particularly when there was nothing to be done or said. (Crossing the Bridge: A Jungian Approach to Adolescence, Translation by Karen Schneider. La Salle: Open Court. 1990, pp.143 -144.)
Do keep in mind that the majority of people will be fine after exposure to a trauma. People who have felt safe and secure prior to the event often have reserves of resiliency to draw upon. Generally, people will be 'shook up' and in shock, then feelings of disbelief, horror, grief and rage may appear. Initially, there may be a preserverative quality about the thought processes, wherein it is impossible to think about anything else. Many clients are reporting 'flashbacks' of the images they saw on television as they try to fall asleep. Sleep may be impacted, and nightmares may occur. Both children and adults may be regressed, with clingy behavior, bedwetting, and a need to stay literally 'in touch' with family and friends. For most children and adults these heightened feelings will diminish in time. We will always remember. The September 11 Terrorist bombing will be marked in the psyche of the nation as much as Pearl Harbor was, or Kennedy's assassination. We will always know where we were when we heard the news.

Colety, age 9
How do we best
treat trauma?
The First 24- 48 hours
ACCORDING TO THE INTERNATIONAL CRITICAL
INCIDENT STRESS FOUNDATION INC. YOU SHOULD CONSIDER THESE ACTIONS WITHIN THE
FIRST 24 - 48 HOURS OF A TRAUMA:
* Engage in periods of appropriate physical exercise, alternated with relaxation
will alleviate some of the physical reactions.
* Structure your time-keep busy.
* You're normal and having normal reactions -don't label yourself crazy.
* Talk to people -talk is the most healing medicine.
* Be aware of numbing the pain with overuse of drugs or alcohol, you don't need
to complicate this with substance abuse problems.
* Reach out- people do care.
* Maintain as normal a schedule as possible.
* Spend time with others.
* Help your coworkers as much as possible by sharing feelings and checking out
how they are doing.
* Give yourself permission to feel rotten and share your feelings with others.
* Keep a journal, write your way through those sleepless hours.
* Do things that feel good to you.
* Realize those around are under stress.
* Don't make big life changes.
* Do make as many daily decisions as possible which will give you a feeling
of control over your life, i.e. if someone asks you what you want to eat- answer
them even if you're not sure.
* Get plenty of rest.
* Reoccurring thoughts, dreams or flashbacks are normal - don't try to fight
them-they'll decrease over time and become less painful.
* Eat well-balanced and regular meals (even if you don't feel like it.)
* Remember to breathe
Recommendations for Family and Friends of Those Most Severely Impacted by
Post Traumatic Stress:
* Listen Carefully.
* Spend time with traumatized person.
* Offer your assistance and a listening ear if they have not asked for help.
* Reassure them that they are safe.
* Help them with everyday tasks like cleaning, cooking, caring for the family,
minding children.
* Give them private time.
* Don't take anger personally.
* Don't tell anyone that they are "lucky it wasn't worse" -traumatized people
are not consoled by those statements. Instead, tell them that you are sorry
such an event has occurred and you want to understand and assist them.
PREPAREDNESS:
Be prepared. Studies show that being prepared actually helps to lessen PTSD
and Trauma Symptoms and helps provide a sense of control and comfort.
* Be aware of surroundings
* Use Common Sense
* Keep emergency phone numbers handy
* Discuss safety techniques with family, friends, neighbors
* Develop and family disaster plan
* Discuss how to protect yourself in case of disaster
* Look at and learn about utility shutoffs.
* Delegate responsibilities
* Plan for special needs (infants, elderly)
* Instruct children how to call emergency numbers
* Re-read first aid training information.
* Draw a floor plan of your house with food, supplies, tools, batteries etc
located on it.
* Practice evacuation.
* Determine 2 or 3 remote "safe- reunion" spots
* Where do your children go if they are away from home and something happens?
* Identify an out of town contact or friend to coordinate reunion efforts.
* Share your plan
* Check your earthquake kit- do you have food, water, flashlights, radios, batteries,
first aid supplies, fire extinguishers, waterproof matches, blankets, shoes
, clothes, diapers, toilet paper, necessary over the counter and prescription
medications, money
* Stay calm
* Reach out to neighbors. Collaborate. Be kind to one another.
FEMA Offers Advice On How To Talk
To Children About Terrorist
Attacks
Washington, D.C., September 12, 2001
 The
terrorist events in New York
and Washington, D.C., have not spared the children of the
The
terrorist events in New York
and Washington, D.C., have not spared the children of the
nation, said Joe M. Allbaugh, director of the Federal Emergency
Management Agency (FEMA). They have seen the terrible television
pictures and heard the adults in their lives discussing the tragic events.
Yet many adults don't know how to talk to children about the
disaster, or don't know how to recognize that their children are
feeling distress.
"Children affected by disasters may suddenly act younger than they
are or may appear stoic - not crying or expressing concern," said
Holly Harrington, the FEMA for Kids manager. "Parents can help their
children by talking to them, keeping them close and even
spoiling them for a little while. We also advise that children not be
overexposed to the news coverage of the terrorist events."
Talking to children about terrorism can be particularly problematic
since providing them with safety guidelines to protect themselves from terrorism
is difficult. According to psychologists, questions about
terrorism are teaching opportunities. Adults should answer
questions about terrorism by providing understandable information and
realistic reassurance. And children don't need to be
overwhelmed with information, so less is better than more in terms of
details.
http://www.fema.gov/nwz01/nwz01_99.htm
Pedro, age 10
Lance, age 9
|
After a Disaster: How to
Help Child Victims
(source: http://www.fema.gov/kids/tch_aft.htm) |
|
On Fear and Fearlessness Going beyond fear begins when we examine our fear: our anxiety, nervousness,concern, and restlessness. If we look into our fear, if we look beneath its veneer, the first thing we find is sadness, beneath the nervousness. Nervousness is cranking up, vibrating, all the time. When we slow down, when we relax with our fear, we find sadness, which is calm and gentle. Sadness hits you in your heart, and your body produces a tear. Before you cry, there is a feeling in your chest and then, after that, you produce tears in your eyes. You are about to produce rain or a waterfall in your eyes and you feel sad and lonely, and perhaps romantic at the same time. That is the first tip of fearlessness, and the first sign of real warriorship... The ideal of warriorship
is that the warrior should be sad and tender, and because of that, the
warrior can be very brave as well. Without that heartfelt sadness, bravery
is brittle, like a china cup. If you drop it, it will break or chip. |
| Helping
the Child or Adolescent Trauma Survivor Author: National Institute of Mental Health Date: September 2001 Early intervention to help children and adolescents who have suffered trauma from violence or a disaster is critical. Parents, teachers and mental health professionals can do a great deal to help these youngsters recover. Help should begin at the scene of the traumatic event. According to the National Center for Post-Traumatic Stress Disorder of the Department of Veterans Affairs, workers in charge of a disaster scene should: -- Find ways to protect children from further harm and from further exposure to traumatic stimuli. If possible, create a safe haven for them. Protect children from onlookers and the media covering the story. -- When possible, direct children who are able to walk away from the site of violence or destruction, away from severely injured survivors, and away from continuing danger. Kind but firm direction is needed. -- Identify children in acute distress and stay with them until initial stabilization occurs. Acute distress includes panic (marked by trembling, agitation, rambling speech, becoming mute, or erratic behavior) and intense grief (signs include loud crying, rage, or immobility). -- Use a supportive and compassionate verbal or non-verbal exchange (such as a hug, if appropriate) with the child to help him or her feel safe. However brief the exchange, or however temporary, such reassurances are important to children. After violence or a disaster occurs, the family is the first-line resource for helping. Among the things that parents and other caring adults can do are: -- Explain the episode of violence or disaster as well as you are able. -- Encourage the children to express their feelings and listen without passing judgment. Help younger children learn to use words that express their feelings. However, do not force discussion of the traumatic event. -- Let children and adolescents know that it is normal to feel upset after something bad happens. -- Allow time for the youngsters to experience and talk about their feelings. At home, however, a gradual return to routine can be reassuring to the child. -- If your children are fearful, reassure them that you love them and will take care of them. Stay together as a family as much as possible. -- If behavior at bedtime is a problem, give the child extra time and reassurance. Let him or her sleep with a light on or in your room for a limited time if necessary. -- Reassure children and adolescents that the traumatic event was not their fault. -- Do not criticize regressive behavior or shame the child with words like "babyish." -- Allow children to cry or be sad. Don't expect them to be brave or tough. -- Encourage children and adolescents to feel in control. Let them make some decisions about meals, what to wear, etc. -- Take care of yourself so you can take care of the children. When violence or disaster affects a whole school or community, teachers and school administrators can play a major role in the healing process. Some of the things educators can do are: -- If possible, give yourself a bit of time to come to terms with the event before you attempt to reassure the children. This may not be possible in the case of a violent episode that occurs at school, but sometimes in a natural disaster there will be several days before schools reopen and teachers can take the time to prepare themselves emotionally. -- Don't try to rush back to ordinary school routines too soon. Give the children or adolescents time to talk over the traumatic event and express their feelings about it. -- Respect the preferences of children who do not want to participate in class discussions about the traumatic event. Do not force discussion or repeatedly bring up the catastrophic event; doing so may re-traumatize children. -- Hold in-school sessions with entire classes, with smaller groups of students, or with individual students. These sessions can be very useful in letting students know that their fears and concerns are normal reactions. Many counties and school districts have teams that will go into schools to hold such sessions after a disaster or episode of violence. Involve mental health professionals in these activities if possible. -- Offer art and play therapy for young children in school. -- Be sensitive to cultural differences among the children. In some cultures, for example, it is not acceptable to express negative emotions. Also, the child who is reluctant to make eye contact with a teacher may not be depressed, but may simply be exhibiting behavior appropriate to his or her culture. -- Encourage children to develop coping and problem-solving skills and age-appropriate methods for managing anxiety. -- Hold meetings for parents to discuss the traumatic event, their children's response to it, and how they and you can help. Involve mental health professionals in these meetings if possible. Most children and adolescents, if given support such as that described above, will recover almost completely from the fear and anxiety caused by a traumatic experience within a few weeks. However, some children and adolescents will need more help perhaps over a longer period of time in order to heal. Grief over the loss of a loved one, teacher, friend, or pet may take months to resolve, and may be reawakened by reminders such as media reports or the anniversary of the death. In the immediate aftermath of a traumatic event, and in the weeks following, it is important to identify the youngsters who are in need of more intensive support and therapy because of profound grief or some other extreme emotion. Children and adolescents who may require the help of a mental health professional include those who show avoidance behavior, such as resisting or refusing to go places that remind them of the place where the traumatic event occurred, and emotional numbing, a diminished emotional response or lack of feeling toward the event. Youngsters who have more common reactions including re-experiencing the trauma, or reliving it in the form of nightmares and disturbing recollections during the day, and hyperarousal, including sleep disturbances and a tendency to be easily startled, may respond well to supportive reassurance from parents and teachers. Reprinted with permission of NIMH |
Crisis Intervention
|
Crisis Intervention:
A Review
An ability
to share the negative emotional impact of a This suffering
suggests the need for preventive and
[International Journal of Emergency Mental Health, 2000, 2(2), 119-125]. http://www.icisf.org/Acrobat%20Documents/TerrorismIncident/CrsIntRev.PDF |
For training in Critical Incident Stress Management please go to: http://www.icisf.org/classofferings.htm
The American Red Cross needs volunteers, and will provide training. If you
can, give blood. Go to:

http://www.redcross.org/donate/volunteer/
for more information.
The Green Cross Projects (GCP) is a humanitarian service
organization originally started by the Traumatology Institute in
response to the Oklahoma City bombing in 1995. The goal of
GCP is to provide immediate trauma intervention to all areas of
our world when a crisis occurs. This includes assistance in the
most recent world disaster, the issue of violence in the media,
the crisis in Kosovo and discussions on other events, such as
the rampage tragedy in Littleton, Colorado (USA). For the most
recent information, other than this web site, members are urged
to read the most recent issue of the e-journal,
TRAUMATOLOGYe and the Newsletter. http://www.greencross.org/
2.
How to Assess for Impact
While we can never generalize about who will be traumatized by an event, there are indicators to assess the possible risk for subsequent Post Traumatic Stress Disorder (PTSD).
Factors to take into account include:
Physical proximity
A child or adult at 'ground zero' of a disaster is more at risk for trauma. If you were in the World Trade Center, escaping for your life, you will be more affected than those who witnessed it, or saw it on TV. This correlates with to Earth, First Chakra Trauma, in which an individual's life was threatened.
Extrapolating from Children’s Responses to Terrorism by Lawrence B. Rosenfeld (source:http://www.naswdc.org/terror/rosenfeld.htm), it may be helpful to envision at "Circles of Vulnerability" in the assessment of trauma. Rosenfeld postulates that the closer a child was to the center of the circle, the more vulnerable he or she is. Therefore, those who witnessed the event, but whose lives were not threatened, would be slightly less vulnerable. Rosenfeld's third circle is those who were in proximity to the disaster, but did not witness it, and his fourth circle is those who heard of the event, saw it on TV, but were not there.
Psychological Proximity
The people in this circle would be those who had a deep connection to someone who was at the disaster; for example, a child whose parent worked at the World Trade Center, a mother whose daughter lived in the area of the Oakland Firestorm. While these people's lives where not threatened, they experienced intense fear and anxiety for people they loved. Distant relatives, or having a 'degree of separation' from someone in the disaster would be the second circle of vulnerability, with circles rippling out from the center to encompass 'those like me'. An example of this would be a child whose parent travels for business; that child might feel closer to risk than someone who did not have a family member who tflies a lot. The circles would hopefully expand to include all humankind. For healing can only happen for the planet if we can each find our "I art Thou" moment. This is the beginnings of true empathy, where we are one.
Past Trauma
Similar Events: The more trauma a person has experienced the more prone they are to being re-traumatized. A veteran or firefighter would be more at risk for flashbacks if he or she had been in a similar disaster. A person who has been in an earthquake will be more stressed and reactive to another earthquake than one who has not. Someone who survived a deadly fire will react more to the smell of smoke than someone who had only seen the fire on TV.
Past Traumas, unrelated: If someone has had past trauma, unrelated to to the disaster they too will be more vulnerable. A sexual abuse victim will tend to be more traumatized than others, as he or she remembers, in a cellular fashion, the feelings of helplessness, vulnerability, rage, grief, etc. Disasters can trigger flashbacks of unrelated trauma as the feelings are aroused.
Age
Generally, trauma is more severe in younger victims. A young child will tend to cognitively 'freeze' the trauma in time. If a child is a preschooler, their primary response, throughout life, will be to view that event though the cognitive and emotional functioning of a preschooler. Subsequent traumas may go back to this level of cognitive development, so, even when faced with a trauma as an adult, they may look and feel like a young child in their processing of the event.
What does PTSD look like in children?
From PTSD in Children
and Adolescents, By Jessica Hamblen, Ph.D. A National Center for PTSD Fact
Sheet.
Researchers and clinicians are beginning to recognize that PTSD may not present
itself in children in the same way as it does in adults (see what is PTSD?).
This can be seen in reviewing the criteria for PTSD which now lists age specific
features for some symptoms.
Very young children may present with few PTSD symptoms. It has been
suggested that this is because eight of the PTSD symptoms require a verbal
description of one's feelings and experiences. Instead, young children may
report more generalized fears such as stranger or separation anxiety, avoidance
of situations that may or may not be related to the trauma, sleep disturbances,
and a preoccupation with words or symbols that may or may not be related to
the trauma. These children may also display posttraumatic play in which they
repeat themes of the trauma in. In addition, children may loose an acquired
developmental skill (such as toilet training) as a result of experiencing
a traumatic event.
Clinical reports suggest that elementary school-aged children may not experience amnesia for aspects of the trauma or visual flashbacks. However, they do experience "time skew" and "omen formation" which is not typically seen in adults. Time skew refers to a missequencing of trauma related events when recalling the memory. Omen formation is a belief that there were warning signs that predicted the trauma. As a result, children often believe that if they are alert enough they will recognize warning signs and avoid future traumas.
School aged children
also reportedly exhibit posttraumatic play or reenactment of the trauma in
play, drawings, or verbalizations. Posttraumatic play is distinguished from
reenactment in that posttraumatic play involves compulsively repeating some
aspect of the trauma, is a literal representation of the
trauma, and does not tend to relieve anxiety (e.g., an increase in shooting
games after exposure to a school shooting) while posttraumatic reenactment
is more flexible and involves behaviorally recreating aspects of the trauma
(e.g., carrying a weapon after exposure to violence).
PTSD in adolescents may begin to more closely resemble PTSD in adults.
However, there are a few features that have been shown to differ. As discussed
above, children may engage in traumatic play following a trauma. Adolescents
are more likely to engage in traumatic reenactment in which they incorporate
aspects of the trauma into their daily lives. In addition, adolescents are
more likely than younger children or adults to exhibit impulsive and aggressive
behaviors. (http://www.ncptsd.org/facts/specific/fs_children.html)
|
|
VIOLENCE IN THE PRESCHOOL YEARS
Children growing up with violence are at risk for pathological development. According to Erikson's classical exposition of individual development, learning to trust is the infant's primary task during the first year of life. Trust provides the foundation for further development and forms the basis for self-confidence and self-esteem. The baby's ability to trust is dependent upon the family's ability to provide consistent care and to respond to the infant's need for love and stimulation. Caregiving is compromised when the infant's family lives in a community racked by violence and when the family fears for its safety. Parents may not give an infant proper care when their psychological energy is sapped by efforts to keep safe (Halpern, 1990). Routine tasks like going to work, shopping, and keeping clinic appointments take careful planning and extra effort. When infants reach toddlerhood they have an inner push to try newly gained skills, such as walking, jumping, and climbing. These skills are best practiced in parks and playgrounds, not in crowded apartments. But young children who live in communities racked by crime and menaced by gangs are often not permitted to be out-of-doors. Instead, they are confined to small quarters that hamper their activities, and that lead to restrictions imposed by parents and older family members (Scheinfeld, 1983). These restrictions, which are difficult for toddlers to understand and to obey, can lead in turn to disruptions in their relationships with the rest of the family.
During the preschool years, young children are ready to venture outside of the family in order to make new relationships and learn about other people (Spock, 1988). However, when they live in neighborhoods where dangers lurk outside, children may be prevented from going out to play or even from accompanying older children on errands. In addition, preschoolers may be in child care programs that are located in areas where violent acts occur frequently.
VIOLENCE: THE SCHOOL YEARS
Although the early years are critical in setting the stage for future development, the experiences of the school years are also important to children's healthy growth. During the school years, children develop the social and academic skills necessary to function as adults and citizens; violence at home or in the community takes a high toll.
* When children's energies are drained because they are defending themselves against outside dangers or warding off their own fears, they have difficulty learning in school (Craig, 1992). Children traumatized by violence can have distorted memories, and their cognitive functions can be compromised (Terr, 1983).
* Children who have been victimized by or who have seen others victimized by violence may have trouble learning to get along with others. The anger that is often instilled in such children is likely to be incorporated into their personality structures. Carrying an extra load of anger makes it difficult for them to control their behavior and increases their risk for
resorting to violent action.
* Children learn social skills by identifying with adults in their lives. Children cannot learn nonaggressive ways of interacting with others when their only models, including those in the media, use physical force to solve problems (Garbarino et al., 1992).
* To control their fears, children who live with violence may repress feelings. This defensive maneuver takes its toll in their immediate lives and can lead to further pathological development. It can interfere with their ability to relate to others in meaningful ways and to feel empathy. Individuals who cannot empathize with others' feelings are less likely to
curb their own aggression, and more likely to become insensitive to brutality in general. Knowing how some youths become emotionally bankrupt in this way helps us understand why they are so careless with their own lives and with the lives of others (Gilligan, 1991).
* Children who are traumatized by violence may have difficulty seeing themselves in future roles that are meaningful. The California school children who were kidnapped and held hostage in their bus were found to have limited views of their future lives and often anticipated disaster (Terr, 1983). Children who cannot see a decent future for themselves
have a hard time concentrating on present tasks such as learning in school and becoming socialized.
* Children need to feel that they can direct some part of their existence, but children who live with violence learn that they have little say in what happens to them. Beginning with the restrictions on autonomy when they are toddlers, this sense of helplessness continues as they reach school age. Not only do they encounter the constraints that all children do, but their freedom is restricted by an environment in which gangs and drug dealers control the streets.
* When children experience a trauma, a common reaction is to regress to an earlier stage when things were easier. This regression can be therapeutic by allowing the child to postpone having to face the feelings aroused by the traumatic event. It is a way of gaining psychological strength. However, when children face continual stress they are in
danger of remaining psychologically in an earlier stage of development.
INDIVIDUAL DIFFERENCES AND RESILIENCE
Not all children respond to difficult situations in the same way; there are many factors that influence coping abilities, including age, family reaction to stress, and temperament. Younger children are more likely to succumb to stress than school-age children or adolescents. Infants can be shielded from outside forces if their caregivers are psychologically
strong and available to the baby. Children who live in stable, supportive homes have a better chance of coping because they are surrounded by nurturing adults. If grown-ups are willing to listen to children's fears and provide appropriate outlets for them, children are better
able to contend with the difficulties in their lives. Children are more resilient if they are born with easy temperaments and are in good mental health. If they are lucky enough to have strong parents who can withstand the stresses of poverty and community violence, children also have a better chance of growing into happy and productive adults (Garmezy & Rutter, 1983).
ADAPTABILITY IN CHILDREN
Although what happens to them in the early years is very important, many children can overcome the hurts and fears of earlier times. For children living in an atmosphere of stress and violence, the ability to make relationships and get from others what they miss in their own families and communities is crucial to healthy development. The staff in schools, day care centers, and recreational programs can be resources to children and offer them
alternative perceptions of themselves, as well as teaching them skills for getting along in the world. With time, effort, and skill, caregivers can provide children with an opportunity to challenge the odds and turn their lives in a positive direction.
Bell, C. (1991). Traumatic Stress and Children in Danger. JOURNAL OF HEALTH CARE FOR THE POOR AND UNDERSERVED 2(1): 175-188. Carnegie Corporation of New York. (1994). Saving Youth from Violence. CARNEGIE QUARTERLY 39(1, Winter): 2-5.
Craig, S.E. (1992). The Educational Needs of Children Living with Violence. PHI DELTA KAPPAN 74(1, Sep 10): 67-71. EJ 449 879.
Garbarino, J., N. Dubrow, K. Kostelny, and C. Pardo. (1992). CHILDREN IN DANGER: COPING WITH THE CONSEQUENCES OF COMMUNITY VIOLENCE. San Francisco: Jossey-Bass. ED 346 217. Not available from EDRS.
Garmezy, N. and M. Rutter, Eds. (1983). STRESS, COPING, AND DEVELOPMENT IN CHILDREN. New York: McGraw Hill.
Gilligan, J. (1991). Shame and Humiliation: The Emotions of Individual and Collective Violence. Paper presented at the Erikson Lectures, Harvard University, Cambridge, MA, May 23.
Halpern, R. (1990). Poverty and Early Childhood Parenting: Toward a Framework for Intervention. AMERICAN JOURNAL OF ORTHOPSYCHIATRY 60(1, Jan): 6-18.
Kotlowitz, A. (1991). THERE ARE NO CHILDREN HERE. New York: Doubleday.
Scheinfeld, D. (1983). Family Relationships and School Achievement among Boys in Lower-Income Urban Black Families. AMERICAN JOURNAL OF ORTHOPSYCHIATRY 53(1, Jan): 127-143.
Spock, B. (1988). DR. SPOCK ON PARENTING. NY: Simon & Schuster.
Terr, L. (1983). Chowchilla Revisited: The Effects of Psychic Trauma Four Years after a Schoolbus Kidnapping. AMERICAN JOURNAL OF PSYCHIATRY 140: 1543-1550.
Wallach, L. (1993). Helping Children Cope with Violence. YOUNG CHILDREN 48(4, May): 4-11. EJ 462 996. Zero To Three. (1992). CAN THEY HOPE TO FEEL SAFE AGAIN?:
THE IMPACT OF COMMUNITY VIOLENCE ON INFANTS, TODDLERS, THEIR PARENTS AND PRACTITIONERS. Arlington, VA: National Center for Clinical Infant Programs. ED 352 161.
Zinsmeister, K. (1990). Growing Up Scared. ATLANTIC MONTHLY 256(6, Jun): 49-66.
(source:Violence and Young Children's Development. ERIC Digest. http://www.ed.gov/databases/ERIC_Digests/ed369578.html)
Sensitivity and Temperament
Individuals vary enormously in how they function in the world. Some people have more sensitive nervous systems, some process information more intellectually than others, etc. You may see two children from the same family, faced with the same disaster, and they may have totally different responses to what has occurred.
Don't underestimate the children!!! They know what is going on. Every child I saw, even the ones as young as three years old, knew that something bad, and something very real had happened. The children I saw ranged from those who did not see anything on TV to those who were weaned on violent media images--every one of them knew what had happened. They could see the reactions in the adults around them, and, as one charming nine year old told me, "Of course I knew it was real. It was on all the channels." For many adults the initial reaction was one of unreality, or that, "It was like something out of a Tom Clancey novel." Yet we don't assume these adults can't differentiate violent movies from violent truth.
Even babies are sensing that something is wrong. In consultations regarding infants, every parent reported disturbances in the baby's behavior, sleep pattern, eating, etc. Further discussion revealed that the parents themselves were feeling very vulnerable; powerless to protect their new babies from evil. They were asking themselves what kind of world would their children inherit. Would they survive to adulthood? The babies were sensing a 'disturbance in the field'. As the parents were feeling reverberations in their psyches, the infants felt that and reacted.
Martin, age 9
3. After the Disaster
Many children and adults are getting worse, now, one month after the terrorist attack. We feel so alone in our feelings. It is if everyone is trying to make it go away by not talking about it; yet, we are flooded with grief and anxiety. Many teachers are saying that the best thing is "for children to get back to the regular schedule". They send home notices that while they will answer questions, they will not raise the topic in the classroom. This is sad, as we have all been wounded by the attack, so we can be healed together if we are able to share our experiences.
Many adults are not able to put into words what they feel. The country is still in shock and grief; fear and anxiety are pervasive, and we don't really have the tools as a culture to enable the healing cycle to deepen. It is too soon for words for many. We need symbols, yet they are hard to find. The prominence of the flag appearing is for some a healing symbol; yet, for others it is an ambivalent image, bringing up memories of protesting the war in Vietnam, or fears of a new war. Religious symbols of healing may be similarly divisive in today's culture.
Probably the best thing to do in our practices is wait, and when a healing symbol appears from the psyche, to notice it. Listen and watch carefully for metaphor and symbolic content. Often this is the unconscious providing healing symbols in an attempt at mastery. When 11 year old Joey wants to talk about Barry Bonds hitting home run number 73, he is probably not only talking about baseball, but about a place where there are rules and heroes, and "the guy without drugs can beat the guy who took drugs". When a young teenager wants to watch horror movies, perhaps she is finding an external expression of the horror within, or the horror in the world. If an adult is talking about the garden, perhaps it is a metaphor for a safe place, the 'temenos' or sacred grove where healing can occur. If someone comes in wanting to talk about replacing his little car for an SUV, perhaps he wants to feel bigger and safer on the road, or have a way to get his family out of the city, into the hills where he needs a four wheel drive.
Notice the metaphors, and do not interpret them. If you can simultaneously hold the metaphor and the deeper meaning, this will establish a resonance. The client will feel held and met, without being made overly self-conscious about the metaphor; perhaps not even realizing it is a metaphor. Sandplay Therapy founder Dora Kalff spoke of this as a 'synchronous moment' between therapist and client. It is far more effective to stay in the symbolic language, trusting that the material will come to consciousness when the person is ready.
|
After the Disaster: A Children's
Mental Health Checklist |

Carol, age 9
| Identifying
At-Risk Children Signs to look for: Withdrawn/quiet - holds head down, lack of eye contact, look of defeat, social isolation What to do: Respect the child's need to be quiet; try to find "a way in," consider cultural difference around eye contact, tell the child it is difficult to hear when their head is down; ask another child to respond to isolated child. Overly responsible/parental - caretaking everyone, doesn't discuss own feelings, straight A student who worries about F's; latchkey children. What to do: Give the child permission and encouragement to play; acknowledge caretaking abilities and ask what can be done for him/her; identify feelings in group and own or other's feelings. Hyper - No focus at all, can't sit still; distinction between high energy and hyperactivity. What to do: Child can leave group briefly to run around the track; give task while in group; child may be removed and worked with individually. Edgy, jumpy - Quick to anger, hypervigilant about others opinions of self, quick to cry What to do: Reflect child's angry feeling, model verbalizing feelings, notice and acknowledge anxiety of others' reactions to self, reflect these feelings to group, allow tears to complete then ask questions. Vying for attention - Raises hand at every question, constantly interrupts others, have name on blackboard for talking too much. What to do: Acknowledge child's enthusiasm and your desire to hear from him/her, explain need to hear others, stop interruptions in progress, acknowledge importance of child's input. Flat affect - Attitude of non-caring, little range in voice tone or volume. What to do: Be animated, but not too excitable, speak in animal voices and ask child to do same, talk about how other people learn to not care Out of control behavior - Little or no respect for authority/limits, lashing out at others What to do: Set clear limits and realistic consequences, follow through with consequences, give child respect. |
FEMA has on-line How to Help Children After a Disaster: A Guidebook for Teachers
http://www.fema.gov/kids/tch_help.htm
Signs and Symptoms of Critical Incident Stress
Tragedies, deaths, serious injuries, hostage situations, threatening situations -
these events are known as "Critical Incidents." People who respond to emergencies
encounter highly stressful events almost every day. Sometimes an event is so
traumatic or overwhelming that emergency responders may experience significant
stress reactions.
The Critical Incident Stress Debriefing (CISD) process is specifically designed to
prevent or mitigate the development of post-traumatic stress among emergency
services professionals.
Critical Incident Stress Management (CISM) represents an integrated "system" of
interventions which is designed to prevent and/or mitigate the adverse psychological
reactions that so often accompany emergency services, public safety, and disaster
response functions. CISM interventions are especially directed towards the mitigation
of post-traumatic stress reactions.
SIGNS AND SYMPTOMS OF CRITICAL INCIDENT STRESS table.
| Physical* | Cognitive | Emotional | Behavioral |
| chills | confusion | fear | withdrawal |
| thirst | nightmares | guilt | antisocial acts |
| fatigue | uncertainty | grief | inability to rest |
| nausea | hypervigilance | panic | intensified pacing |
| fainting | suspiciousness | denial | erratic movements |
| twitches | intrusive images | anxiety | change in social activity |
| vomiting | blaming someone | agitation | change in speech patterns |
| dizziness | poor problem solving | irritability | loss of or increase in appetite |
| weakness | poor abstract thinking | depression | hyperalert to environment |
| chest pain | poor attention/ decisions | intense anger | increased alcohol consumption |
| headaches | poor concentration/memory disorientation of time, place or person | apprehension | change in usual communications |
| elevated BP | difficulty identifying objects or people heightened or lowered alertness | emotional shock | etc... |
| rapid heart rate | increased or decreased awareness of surroundings | emotional outbursts | |
| muscle tremors | etc... | feeling overwhelmed | |
| grinding of teeth | loss of emotional control | ||
| shock symptoms | inappropriate emotional response | ||
| visual difficulties | etc... | ||
| profuse sweating | |||
| difficulty breathing | |||
| etc... |
* Any of these symptoms may indicate the need for medical evaluation. When in doubt, contact a physician.
source:http://www.icisf.org/CIS.html
International Critical Incident Stress
Foundation, Inc.
10176 Baltimore National Pike, Unit 201
Ellicott City, MD 21042
Handouts for Patients
The American Red Cross offers printable brochures on the following topics:
How Do I Deal With My
Feelings?
Disasters create an abrupt change in reality. Following the attacks on the World
Trade Center
and the Pentagon, for thousands and thousands of people, reality now includes
the loss of
loved ones—spouses, significant others, children, other relatives, friends,
and neighbors.
Helping Young Children
Cope with Trauma
Disasters are upsetting to everyone involved. For a child, his or her view of
the world as a safe
and predictable place is temporarily lost. Children become afraid that the event
will happen
again and that they or their family will be injured or killed.
When Bad Things Happen
The recent terrorist attacks may have caused you to question a number of things
you have
always believed about your own safety, and the safety of your family and friends.
Why Do I Feel Like This?
There are two types of disaster: natural disasters like the damage that results
from a hurricane,
a tornado, floods, forest fires, volcanoes erupting and earthquakes, and disasters
that result
from an intentional action of a human. When the disaster is human caused, our
reactions are
more severe and become much more complicated and difficult to overcome.
These are available
on-line as:
Printable Version in English...
Printable Version in Spanish...
Printable Version in Farsi...
Printable Version in Laotian...
Printable Version in Cambodian...
Printable Version in French...
Printable Version in Korean...
Printable Version in Tagalog...
Printable Version in Vietnamese...
Printable Version in Russian...
Printable Version in Chinese...
Printable Version in Arabic...
at http://www.redcross.org/services/disaster/keepsafe/attack.html
Acute Stress Disorder and Post-traumatic Stress Disorder
While the focus of the clinical examples in this course is the Terrorist attack of September 11, Acute Stress Disorder (ASD) and Post-Traumatic Stress Disorder (PTSD) can develop from a myriad of causes. People that have been sexually abused, raped, assaulted or physically abused are one category of people with stress disorders often seen in psychotherapy. Those who have had severe illness or medical interventions likewise may manifest PTSD. I have seen PTSD following infertility treatments, surgeries for breast cancer, in children with cancer, etc.
There are times when a whole community
is at risk for ASD and PTSD, such as in the Bay Area following the Loma Prieta
Earthquake, and in communities following catastrophic natural disasters, such
as hurricanes, typhoons, mudslides, floods, volcanic eruptions., etc. War can
cause PTSD, as can acts of aggression against an ethnic group or followers of
a religion. According to an abstract of
The Terrorist Bombing in Oklahoma City by Sitterle and Gurwitch,
When compared to natural disasters, the magnitude and severity of
emotional difficulties are likely to be far greater in response to
terrorist incidents. This is especially true of terrorist incidents that
involve large numbers of fatalities, including the deaths of many
children, are the result of deliberate acts of violence, and involve a
protracted rescue and recovery effort. (source: http://dciswww.dartmouth.edu:50080/v3?db=105&page=q&qry=
Topic%20%22%20terrorist%22&dfn=2&srt=-1)
Perhaps we should look to Israel or Ireland to see how a population handles terrorism, as the examples in the US are fortunately few. The opportunity we have is healing at a national level, as the hurting was done to us all.
Initially, many people will manifest signs of Acute Stress Disorder. Immediately after a trauma, you can not use the diagnosis of Post-Traumatic Stress Disorder, as PTSD requires that "Duration of the disturbance (symptoms in Criteria B, C, and D) is more than 1 month." So a more appropriate diagnosis initially is that of 308.3 Acute Stress Disorder
|
308.3 Acute Stress Disorder
C.The traumatic event is persistently
reexperienced in at least one of the following ways: recurrent images,
thoughts, dreams, illusions, flashback episodes, or a sense of reliving
the experience; or distress on exposure to reminders of the traumatic
event. Differential Diagnosis American Psychiatric Association
(1994). The diagnostic |
What is Post-Traumatic Stress Disorder?
A National Center for PTSD Fact
Sheet
Post-Traumatic Stress Disorder, or PTSD, is a psychiatric disorder that
can occur following the experience or witnessing of life-threatening
events such as military combat, natural disasters, terrorist incidents,
serious accidents, or violent personal assaults like rape. People who
suffer from PTSD often relive the experience through nightmares and
flashbacks, have difficulty sleeping, and feel detached or estranged, and
these symptoms can be severe enough and last long enough to
significantly impair the person’s daily life.
PTSD is marked by clear biological changes as well as psychological
symptoms. PTSD is complicated by the fact that it frequently occurs in
conjunction with related disorders such as depression, substance abuse,
problems of memory and cognition, and other problems of physical and
mental health. The disorder is also associated with impairment of the
person’s ability to function in social or family life, including
occupational instability, marital problems and divorces, family discord,
and difficulties in parenting.
(source: http://www.ncptsd.org/facts/general/fs_what_is_ptsd.html)
|
309.81 Post-traumatic Stress
Disorder American Psychiatric Association
(1994). The diagnostic |
|
Mike's PTSD symptoms, in remission for a while, flooded him. He couldn't sleep, and when he did sleep, he was haunted by violent nightmares, often waking up drenched in sweat. He was agitated and restless. The war starting brought back severe anxiety and depression, as well as flashbacks. While Mike had so far resisted using drugs and alcohol for self-medication, I feared that the risks of a relapse were extremely high. I felt that therapy, even twice a week, was not sufficient. Mike agreed to go back to AA, and took two referrals; one to a psychiatrist for medication, and one to the Veteran's Administration for a group of veterans that focused on PTSD. I knew my limitations..that Mike needed to talk out and relive his combat experiences with someone who had been there. At first he resisted the psychiatric referral, saying that in the past his AA sponsors had frowned upon the use of medication. He finally agreed to give it a try, particularly if we looked at it as possibly a short term intervention. For Mike, the terrorist attack in combination with the war starting were too much; his psychological homeostasis was threatened. The unresolved trauma of serving in Vietnam triggered the present time stress reaction. I was very glad that he took the referrals, particularly to the group experiences of AA and the PTSD group, as Mike had been too often alone and isolated in his suffering. |
Excerpted from A MINI-COURSE FOR
CLINICIANS AND TRAUMA WORKERS
ON POSTTRAUMATIC NIGHTMARES
By Alan Siegel, Ph.D.
Common nightmare themes
1) falling
2) being chased or kidnaped (animal chasing are more common in children)
3) rejection, abandonment, betrayal, or humiliation
4) natural disasters: earthquakes, tidal waves, tornadoes, floods
5) technological disasters such as explosions, fire, nuclear war and chemical
contamination, plane crashes.
6) violent attack and/or injury to self or others.
7) ghosts returning from the dead in a frightening form
8) cars or planes going out of control or crashing
9) being paralyzed or unable to respond an urgent or life threatening challenge
10) illnesses such as cancer, aids, paralysis
11) mortal threats from attackers, thieves, animals or creatures
How posttraumatic nightmares are
different?
1) PTSD nightmares are more emotionally intrusive and anxiety-provoking.
2)blank or content-less nightmares may occur before the dreamer can tolerate
any recall of the affects connected to the trauma.
3)they may be repetitive and unchanging nightmares with minimal adaptive response
to threats arising within the dream.
4) PTSD nightmares insistently repeat some aspects of the trauma but with some
elements changed or missing. E.g. A wildfire becomes a rageful animal or a murderer
becomes a kidnapper who assaults someone else while the dreamer watches.
5)encapsulation: like a psychological abscess, intolerable emotions and conflicts
linked to the trauma continue to infect the psyche but are walled off from consciousness,
yet persistent in dreams.
6) fading: as a trauma is resolved, there is less fixation on the trauma as
the major theme in dreams and trauma-related conflicts are mixed with current
issues and challenges.
(source: http://www.asdreams.org/magazine/articles/seigel_nightmares.htm)
The Association for the Study of
Dreams has established a
Nightmare Hot Line : They need volunteers to staff the line. Please go to:
http://www.asdreams.org/nightmare_hotline.htm
to help.
What are the Traumatic Stress Effects of Terrorism?
A National Center for PTSD Fact Sheet
Information from past incidents
of terrorism
Fortunately, there have been very few terrorist attacks in the United States.
One implication, however, is that there is little known about how people are
affected by terrorism. A consistent finding is that, while most individuals
exhibit resilience over time, people most directly exposed to terrorist attacks
are at a higher risk to develop PTSD. Problems with anxiety, depression, and
substance use are also commonly reported. Predictors of PTSD include being closer
to the attacks, being injured, or knowing someone who was killed or injured.
Those who watch more media coverage are also at higher risk for PTSD and associated
problems. Research from both domestic and international terroristic events sheds
some light on the heightened risk for traumatic stress reactions in individuals
exposed to these events:
Oklahoma City Bombing
As indicated above, rates of distress and post-traumatic symptoms have been
found to be high in individuals studied following terroristic events. Ultimately,
reducing the risk of traumatic stress reactions is best accomplished by abolishing
trauma in the first place by preventing war, terrorism, and other traumatic
stressors. The next best approach is to foster resilience and bolster support
so that individuals have better coping capacity prior to and during traumatic
stress. The third best option is early detection and treatment of traumatized
individuals to prevent a prolonged stress response.
(source: http://www.ncptsd.org/facts/disasters/fs_terrorism.html)
|
Janelle is 22, but her developmental disabilities give her the cognitive functioning of an early adolescent. In addition to her learning differences, Janelle was sexually abused as a young child. Prior to the September 11 attack, Janelle had been doing remarkably well in her vocational training program, surprising the staff and her family with how well she was coping. After the disaster, she seemed fine, asking appropriate questions about what had happened and expressing some concerns about her personal safety. As the weeks progressed, however, Janelle began to deteriorate. She became clingy and regressed, and her cognitive functioning began to diminish. She was forgetful and distracted, making numerous errors in her tasks as well as her writing and spelling. She appeared overwhelmed at her training school, and would hide for hours in the bathroom. Her posture changed from that of a lovely young woman to someone who shuffled and slumped, peering out from behind uncombed hair. She seemed to be willing herself to disappear before our eyes. In therapy, she kept repeating that she was scared, but did not know why. She seemed about four years old, which was the age when she had been sexually abused. Janelle seemed to be having flashbacks, but it was hard to tell for sure, because she had even lost the word 'flashback' when her emotional and cognitive functioning became so diminished. All she wanted to do in her sessions was play with dolls, while rocking back and forth. It was as if Janelle had time traveled back to her earliest trauma. |
Following the research of Bessel A. van der Kolk and Rita Fisler, presented in Dissociation and the Fragmentary Nature of Traumatic memories: Overview and Exploratory Study and their citation of numerous authors on trauma [Janet (1889; van der Kolk & van der Hart, 1991), Kardiner (1941) and Terr (1993)] tends to validate anecdotal reports that memories of trauma live in the senses, and that words come later, if at all. These authors have observed that "trauma is organized in memory on sensori-motor and affective levels.... that 'memories' of the trauma tend to, at least initially, be predominantly experienced as fragments of the sensory components of the event: as visual images, olfactory, auditory, or kinesthetic sensations, or intense waves of feelings ." (source: http://www.trauma-pages.com/vanderk2.htm)
"While our understanding of the mind-body complex may be in its infancy from a scientific perspective, it is becoming increasingly clear that the neurochemistry of emotion is a key factor that must be considered if any therapeutic intervention is to have lasting effect. All memory is encoded at the cellular level." (Decoding Traumatic Memory Patterns At The Cellular Level by Thomas R. McClaskey, D.C., C.H.T., B.C.E.T.S.; The American Academy of Experts in Traumatic Stress at http://www.aaets.org/arts/art30.htm)
This is in alignment with what I have noticed in 25 years of being a therapist, treating a large number of children and adults with PTSD, including those impacted by the 1989 Loma Prieta Earthquake in San Francisco. I have found that the use of the elements (earth, air, fire and water) facilitates the healing of trauma embedded in the chakras or energy centers.
How then do we treat trauma?
It appears that words do not encompass
the range of the terror, nor do they have the power to heal what is held in
the cells and the senses. The Elemental Model for healing incorporates the energetic
system of the Tibetan Buddhists with a technique that engages the cells and
senses through the use of the elements. Rather than a 'new' model, this is actually
an ancient system. The elements often tie into energetic centers in the body
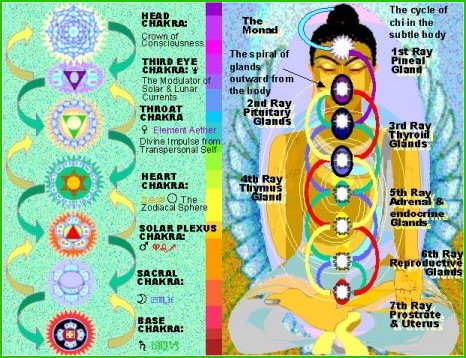
called chakras. The western medical system calls them "nerve plexuses". Each
energy center is a 'sense center' and is correlated with an element. We will
use the Tibetan five point system, rather than the seven chakra system of the
Hindus.
For treatment of post-traumatic stress,
focus is on the lower four chakras. Trauma often impacts very deeply on a victim's
life. After the bodily bruises heal, it is necessary to assist the victim in
healing the mind and spirit if we wish them to not only survive, but to thrive.
| Element | Type of Trauma | Physical Reactions* | Psychological** Reactions | Symbols | Therapeutic Goal |
| Earth:Basic Trust, survival | Life threatening | Life threatening injuries, shock, dissociation | Major depression, suicidal, psychosis, self-destructive behavior | Primitive monsters, catastrophe, being devoured | "I am alive" |
| Water:Attachment | Attachment abuse | Chills, vomiting, GI disorders, anorexia/bulimia | Abandonment fears, feelings of betrayal, lack of trust | Flooding, bathrooms, sharks | "I can trust again" |
| Fire: Heart | Stranger Abuse/loss of a loved one | Hot flashes, rage reactions, heart palpitations | Rage, feelings of disempowerment | Fire, wars, weapons | "I can love again" |
| Air:Communication | Inability to communicate | Difficulty breathing, choked up | Disorientation | Flying, phones | "I can speak again" |
| Ether:Spirit | disorientation, spiritual crises | Headaches, seizures | Spiritual Crisis | Birds, angels, divinity | 'I am" |
**Feelings of initial dissociation, shock, fear and overwhelm may accompany all types of trauma. Alcoholism and addiction may show up at any stage.
Although psychological conflicts
do manifest in the body, please remember the scope of your practice and always
refer to a physician for the monitoring of physical care. We are not stating
that trauma causes illness, but rather that the chakras tend to correlate with
specific organ systems.
It is useful in diagnosis and treatment to look at the type of trauma in relation to chakra system, to determine energetically where the libido is blocked. The chakras correlate to the endocrine system and various nerve plexuses (Tart, 1975), and have emotional and symbolic aspects as well. While there are five chakras (seven in the Hindu system), trauma and its healing usually are limited to the first four; first, the root or survival chakra; second, the sacral plexus or attachment chakra; third, the navel or power chakra and the heart chakra. (Eliade, 1973). The usefulness of the chakra system in a treatment model is that it combines the physical, the emotional, the spiritual and the symbolic, allowing the diagnosis and treatment to be multifaceted and accurate. Trauma in the first three chakras must be addressed before the client reaches the fourth chakra, throat. The plexus here is the pharyngeal region and the region it rules is communication. This is often why the victim must reenact the crime before he or she is able to talk about what happened.
According to Dr. Cecil Burney, a founding member of the International Society for Sandplay Therapy, in Tibet, every illness is viewed as a problem of the heart. Dr. Burney spoke of a Tibetan lama who expressed amazement about Western medicine and psychotherapy. The lama told Dr. Burney, after hearing about Western psychotherapy, "I do not understand this Western way of healing! It is very strangeyou have a person with a problem of the heart; a burning problem, and you have them talk about it. This is just adding air to fire." This refers to the Tibetan belief that all illnesses, whether physical or emotional, are matters of the heart. The element of the heart is fire, and if you talk about a trauma, a feeling or an illness, you are adding air to fire; fanning the flames. The lama told Dr. Burney, "And even worse is when people spiritualize their problems! I never trust people who appear too spiritual. They might be carrying a knife behind their backs." (Cecil Burney, personal communication, 1985. A version of this story appears in Shepherd, S.(1986)
People who have experienced trauma
need to go down. An initial spiritual solution is often a bypass; anger smoldering
under a fragile facade. Yet, to descend means looking at the shadow, getting
angry, and grieving the losses we have experienced in life. Embarking on this
journey takes courage.
The healing of a trauma would involve a descent, to point the triangle of the heart down through the water to the earth. When Dora Kalff taught about the Tibetan chakras, she would draw a diagram with a square at the base, with a circle on top of it. Then there was a triangle, a horizontal crescent, and at the very top was a flame. Frau Kalff told us that these represented the Tibetan chakras, and that each shape correlated to an element and a part of the body. The elements, in ascending order, represented are Earth, Water, Fire, Air and Ether (or Spirit). The lower elements are associated with matter, the soul, and the feminine. The upper elements of air and ether are connected with the spirit and the masculine. The heart in the center is the bridge between the two; uniting feminine and masculine; soul and spirit. (Dora Kalff, personal communication, 1978)
ETHER:SPIRIT
AIR: COMMUNICATION
FIRE: HEART
WATER: ATTACHMENT
EARTH: BASIC TRUST, SURVIVAL
Frau Kalff taught us of the G-Tumno
Tibetan meditation of inner fire. In this meditation, the triangle of the heart
points down.  Burning issues
quiet, as the fire slows. When the fire touches water, mist forms. The tears
flow. When the fire connects to the element earth, the person may feel grounded,
'in touch'. At this moment, when the fire descends to the center of the earth,
there is a natural arcing up of energy. The life force ascends, allowing the
triangle of the heart to simultaneously point upward and downward. In this void
arises the thousand petaled lotus of enlightenment. We also know this shape
as the Star of David, or the "yantra".
Burning issues
quiet, as the fire slows. When the fire touches water, mist forms. The tears
flow. When the fire connects to the element earth, the person may feel grounded,
'in touch'. At this moment, when the fire descends to the center of the earth,
there is a natural arcing up of energy. The life force ascends, allowing the
triangle of the heart to simultaneously point upward and downward. In this void
arises the thousand petaled lotus of enlightenment. We also know this shape
as the Star of David, or the "yantra".
The energetic model of therapy starts with a descent through the elements, and correlates each element with an energy center in the body (chakra) and with a developmental level. Knowing these relationships helps make sense of the very confusing world of the unconscious. Although this information may initially seem complex, we have seen that the elements provide a bridge between the client's psychological, physical and spiritual self, which is readily witnessed in the sandtray.
The descent from one level to the next is through transference tests. If a client does not feel safe, he or she will not go to the next level. The therapist needs to know these levels in him or herself, or the process will not evolve. This is the most common reason we see in our consultation when a therapist says "Joey only plays soldiers - all the time, he does the same tray over and over again". Another reason clients perseverate is that the therapist does not know what is happening and, therefore, fails to empathize. There is also the possibility that the family system is refusing to change, as evidenced by inconsistency in following through or not bringing the client to sessions regularly.
Seth, age 10, played army every week for seven weeks in a row, lighting candles.
This was using the element fire.
Seth
was slated to go visit relatives  out-of-state,
and his anxiety was increasing. The therapist uncovered an incident of inappropriate
sexual contact with an older boy. When this was discussed and interventions
made with the family so this would not be repeated, Seth's sandtrays immediately
changed. He dug down to the blue bottom of the tray and began to add water.
out-of-state,
and his anxiety was increasing. The therapist uncovered an incident of inappropriate
sexual contact with an older boy. When this was discussed and interventions
made with the family so this would not be repeated, Seth's sandtrays immediately
changed. He dug down to the blue bottom of the tray and began to add water.
The model we present can be useful in assessing where the client is in his or her own process. People start at various points. When an idea comes into being it goes through the four elemental planes: air, fire, water, earth. A note of caution here: not every client needs to go through all the elements. Some will go just one or two stages, then ascend. Trust your clients -- they will know when it is time to stop. For the sake of the model we will start with the element ether or spirit.
(The description of the Self and the
elements is from Amatruda and Simpson, Sandplay,The
Sacred Healing: A Guide to Symbolic Process, Trance-Sand-Dance Press: Taos,
1997. Portions of the Elemental Model also appear in that book, as well as in
the Journal of Sandplay Therapy, Archives of Sandplay Therapy, and Psyche &
Soma)
ETHER/SPIRIT
The fifth or crown chakra is located in the at the at the top of the head and center of the forehead and is sometimes called "the third eye". It is where we get a different picture of the world and is associated with the objectivity of air. When we feel someone is trying to force an idea or perspective on us, it will often produce a tension headache.
It is pure spirit: our direct connection to God or higher power. It often is represented by a crown or halo. It is the sensation of a tingling from the top of your head to the bottom of your toes that assures you that you have just had a moment of truth and insight. It is rarely blocked except in the cases where an individual has chosen to give up their personal authority to another dominating human being such as a cult leader.

AIR
Air is the element of the fourth chakra, which is located in the throat, and radiates to the ears. It is where we hear others and our inner voice, where we communicate. When we get "choked up" we often need to let our feelings out and give them voice.
Air enters after an idea has taken form and we are able to stand back and objectively witness it. Air is Logos, the divine, objective principles of universal order. It governs thinking, intellect, objectivity, communication and often change. The wind is the spirit of the unconscious. In the Medicine Wheel it is the direction of the East, the place of our ancestors, where new life begins, and often where therapy begins. The color of the East is yellow, and its animal is the eagle, for clear vision and for the ability to soar and speak to the spirits. The signs of the Zodiac are Gemini (communication), Libra (relationship and balance) and Aquarius (universal brotherhood). The tarot suit is swords or ñs-wordsî which describe how we use thoughts and words to direct our energy and shape our world.
This is clearly an appropriate place for therapy to start. In feelings it is both detachment and anxiety. In sound it is often the music that makes you feel "spaced out", like harps or some New Age music. It is associated with the 4th chakra of communication and perception. In trays it turns up as salvation and escape - feathers, balloons, sailboats, birds in flight, angels, flutes, harps, saxophones, songs, books, sandstorms, hurricanes, tornadoes, tilted figures. It appears white or shiny. It is the "breath of life", called "ba" in Egypt. It "gives voice". When there are people, animals or monsters talking, singing or yelling, there is air. When it is unbalanced it becomes rigid, pedantic, sterile, over intellectualized. It often signals the process of change occurring. It will add fuel to the fire and move loose earth, cause whitecaps on the water. Air signals life; newborns cry.
Developmentally, intimacy vs. isolation
probably bridges both air and water. In adolescence and young adulthood we can
reach out and touch others with ourselves. Do we take the chance to converse
and share healing? Later are we able to call on our "angels" for help? Are we
open to the messenger doves flying in? In disease as isolating as addiction
it is often the communication and fellowship shared with AA and other 12 step
programs that provide the structure and support for recovery and healing.

FIRE
Carrie was wounded in the third, or fire chakra. She came to therapy at age 11, and had been molested by an older boy when she was 7 years old. Her reaction was to deny that it had happened, alternating with periods of severe stomach aches, ruminations about things that disturbed her (i.e., the Children's Crusades in the Middle Ages), as well as outbursts of rage. The chakra impaired was the third, solar plexus and the heart.
The emotional issues of the third chakra are power and love. This girl's growing sense of herself was constrained by the guilt subsequent to the molest. The element associated with this chakra is fire, and indeed she repeatedly lit candles in the sandplay. After she lit the fires, then she could talk about what had happened. During an earlier period of play therapy (with another therapist who did not use sandplay) Carrie had not been able to reach the depths that she descended to in sandplay, nor had she lit fires. In the first therapy, she told only partially of the molest, and her symptoms were only partially alleviated. Because the abuse was not by someone she had trusted, and because her life was not threatened, the obstruction centered around the third chakra. If her history had included previous abuse by a parent, the incident would have impacted the second chakra and possibly the first as well.
Fire in the power chakra "represents the experience of the divine as well as our inner passions". Psychologically, after our baptism into the passions hidden in the deep waters of the unconscious (the second chakra), the third chakra is the experience of emotions flaming up -- "after baptism comes temptation and hell" (Coward, 1985).
Survivors of abuse often have many physical illnesses or injuries during the process of uncovering abuse. Stomach, abdominal and reproductive difficulties (second and third chakra involvement) are common with sexual abuse survivors.
The third chakra is located at the solar plexus and the heart. It is associated with fire, power, reaching out, loving, compassion for self and others as well as the physical body. The third chakra opening makes one feel forceful and intimidating. It is an important chakra to know how to use. The physical sensation can be that of being "hit in the gut". Many of us have had wounds to our hearts when we have taken the risk of loving another and feel we have been burned.
Fire is inspiration. It is the original creative energy. It motivates, inspires, perseveres and destroys. In the Medicine Wheel, this is the direction of the South. It is associated with the color red, the mouse, and the spontaneity of the child. Fire transmutes. The fire signs of the Zodiac are Aries (the beginning ñI amî), Leo (ñI createî) and Sagittarius (ñI teachî). In tarot is the suit of wands which direct the creative force energy to work and become manifest.
Fire will burn until all of its fuel is exhausted. Fire was stolen from the Gods by Prometheus or Coyote in American Indian legend, and children often steal fire from adults. Observe how your child clients relate to fire in the sandtray, notice how confident they are in lighting candles. It is prudent to review fire safety rules with children when they light candles, and to have an obvious bottle of water available should quick extinguishing become necessary. Fire teaches through surprise and opposites. It gives man power over nature. Fire is active and initiates projects. It is associated with the third and fourth energy centers, power and love and compassion.
The colors of fire are reds, oranges,
yellow; the hottest part is often blue. It is the opposite of water. The color
red emotionally is both anger and love. In true love there needs to be room
for the anger. Troubled marriage partners often refer to a lack of spark. They
may not allow anger or disagreement (fire) into their union. Or there may be
so much rage that there is little space for the expression of love. In the tray
we may see light, candles, fire, fire engines, stop signs, volcanoes, cinders,
suns, birthday cakes, ovens, cooking, pipes and fire-colored objects of all
sorts. The sounds would be hissing, crackling, rock and roll.
 BLACKENING
BLACKENING
Blackening is a sub-phase of fire. When something is burnt, it is black. Caregivers that feel witchy are in this stage. The concern and warmth they usually manifest is ñburnt outî. The healing is for them to learn to give more to themselves, to relight their own creative fires. Predominately black trays usually appear when the client feels he or she is in the "dark night of the soul". The energy is spent, there is no inspiration, passion, anger, or love. We have entered the void. Fortunately, there is usually still some small sign of hope in these trays. Try to identify it and see if it may provide the elemental cue as to where the healing will begin, but don't say it. Notice for yourself. Empathize with the pain and the darkness. Clients in the blackening stage may be seriously depressed or suicidal. It is important to honor that, and not attempt to bypass the real pain and despair of the time. Until the darkness is fully recognized the light does not enter.
This is the place where we also confront our own shadow and darkness. Many became so enraged by the act of terrorism on September 11 that they became terrorists in their own hearts, seeking retaliation, retribution, revenge. If we had "bombed Afghanistan back to the stone age" we would have been massacring innocent people, just like what was done to us. Hatred and revenge are aspects of the human psyche that we must acknowledge in ourselves for planetary healing to occur. Honor your shadow, by acknowledging some really horrible part of yourself that it is easier to project onto someone else...this work could save the planet, if everybody did it. Speak out against racial and religious stereotyping!!!
Take some time to root out violence in your own heart, and to understand your
own aggression. If we fearlessly do this, then we make a tiny step toward changing
the consciousness of the world.
![]() REDDENING
REDDENING
There is a process we have noticed in trays we refer to as reddening. There may be an initial reddening to call attention to the difficulty or wound, then the tray gets black. The return to reddening may appear in the form of healing elements. Red is a predominant color at births and menstruation. It is blood, life force. In Chinese culture, red is the color used at weddings and at many other holidays. During the healing phases you may see the red Buddha, or Quan Yin, red candles, or the red cloak around Christ, apples, roses, pomegranates, or other red items that can nourish body and/or soul. Think about how many mythic and fairytale figures encounter red: Persephone, Snow White, Little Red Riding Hood, Dorothy of the Wizard of Oz, Eve, Sleeping Beauty, etc. This healing through reddening often marks a very transformative part of the healing. When the red appears, the client has been touched by Eros, or true feeling. It is life affirming and fertile.
The Erikson developmental levels associated with fire would be industry vs. inferiority, intimacy vs. isolation, generativity vs. stagnation. In an adult, issues around anger, self expression, and procrastination and self fulfillment often revolve and heal around the element of fire. Are they going to express themselves and their souls' desires this lifetime? The therapeutic process should awaken the client's fire, increasing their inspiration and motivation to engage in life.
|
Finally, at the end of the session, it was time to put the fire out, using the cooling waters if the second chakra. Josh was able to reconnect with his feelings of attachment to heal the hurt and anger in his gut and heart. After the session ended, Josh was softer. The vibrating tension in his muscles relaxed. He seemed to melt into his mother's body when she came to pick him up. She seemed surprised by the depth and gentleness of the hug that he gave her.
|

WATER
Second, or attachment chakra trauma often has its roots in betrayal. If a child is sexually abused by a caretaker or parent, the feeling of empathy is damaged. In the body, this can appear as reproductive and urinary tract problems. Behaviorally, a trauma victim will dissociate or not be engaged energetically with the chakras affected by the trauma. When he or she does reintegrate, the symptoms will reflect which chakra has contracted due to the trauma.
When a betrayal takes place, a person is deep in the second chakra "down into the water where the monsters of the deep are faced, and from which rebirth may take place" (Coward, 1985). This is often expressed in sandplay in flooded trays, almost as if the person is feeling as betrayed as humankind must have felt when God flooded the world. The resolution for this often includes a rainbow, symbolizing The Covenant. When this appears, often trust is reestablished.
Water is the element of the second chakra is located below the navel in the abdominal area. Here is the seat of empathy, sexuality and reproduction. Water flows as does empathy and sexuality. When one has been traumatized in this area, the second chakra may develop a physical response. In sexual abuse survivors whose second chakra may have been opened too early and against their will, we often see accompanying issues of gender identity, difficulties with reproductive organs, and problems with trust and attachment to intimate partners.
In the Medicine Wheel water is the element of the West. It signifies introspection and is associated with the color black, the whale, and the bear in the cave. The Zodiac water signs are Cancer (nurturance), Scorpio (release), ending with the mutable water sign of Pisces wherein all is possible, assimilated and given back to spirit.
Water is change. It is where life
begins in the womb, in the ocean. It is the place of dreams, feelings, loss,
love, compassion, empathy, betrayal, cleansing and healing. The tarot suit that
represents water is cups, the vessel from which we express our love. The colors
are blues and greens. If the water is murky, there is emotional confusion around
the issue. It is soothing music or violent storms. We see it in trays as the
blue bottom of the tray itself. It is the unconscious. It can be rivers, ponds,
oceans, streams, ducks, fish, octopi, shells, boats, bridges, sunken treasure,
skin divers, mermaids, pearls, ice, penguins, polar bears, seals, walruses.
When water is out of balance, it floods or there is drought. When water is unrelated,
it freezes; there is no connectedness nor understanding and things appear isolated.
The "monsters from the deep" appear and threaten to overwhelm. Water can erode
valleys, carve mountains, create steam, or put out fire. It cradles intuition
and creativity. It releases and cleanses in tears. For an article on "How
water reflects our
consciousness" please go to http://www.wellnessgoods.com/art_wat_messages.html
Autonomy vs. shame and doubt and
ego integrity vs. despair are Eriksonian stages associated with water. Are we
going to continue to create and give with our body and souls until the end of
life or do we stop and dry up before our time is over? We physically "dry up"
during the process of aging, yet there is little more powerful than the glow
of wisdom in the eyes of an older, vibrant person. A most prominent example
is Mother Teresa who continued to live, share, give and inspire to the end.
At the culmination of therapy a client knows their inner emotions (water) and
has assimilated (water) their soul into action.

EARTH
First chakra trauma is very easy to spot. The client will often appear disoriented and dissociated. They may be in shock. In matching energy, you find yourself spacey and frightened. Survival issues include any incident in which a person's life has been threatened: severe illness, an accident or crime in which a person faced the possibility of death. Veterans of war who exhibit post-traumatic stress disorder often have first chakra disturbances. People with this kind of experience need to descend all the way to the earth in order to heal.
The client's response will often be to repress or deny the traumatic event in order to maintain the integrity of the ego. Exposure to great pain or horror will often create a dissociative reaction, in which the person seems to observe violence rather than experience it. This is essentially a self-protective reaction, a "slipping out of the cocoon" (Kubler-Ross, 1983). The Cherokee would "put their soul in a tree" for protection before they entered battle. Eliana Gil (1987) describes drawings by children who have been violently sexually or physically abused. The pictures show a child being beaten, and in one corner of the paper, high above, a little figure hovers. When asked the child will say that this little figure is him or herself, while the child being abused is "some kid." The bruises on their bodies belie this. The sequelae to this dissociation often includes anxiety, psychosomatic reactions, hyperactivity, regressive behavior, sleep disturbances, trouble concentrating, and constricted or inappropriate affect. In cases of extreme early abuse, multiple personality disorders may develop. The trauma victim often combines the diagnoses of a Dissociative Disorder with that of Post-Traumatic Stress Disorder. There is a seesawing back and forth between dissociating from the event, then being flooded by it. Many adult clients victimized as children will exhibit the same symptomatology, and have within them an inner child who is fragmented and in pain.
How then do we treat the survivor? Encouraging the client to talk about the crime is an important component in therapy, yet too often he or she is unable to put in words what has been experienced. If the person is in a dissociative stage, she or he will, in all honesty, deny that the event has occurred, and if in touch with the incident, in all likelihood is too flooded to give words to what has occurred.
This is where the use of the elements and of sandplay therapy excels as a therapeutic treatment. The sandbox and toys give clients a chance to tell, without words, their own story. Because the world is outside the box, the box and the receptive presence of the therapist provide the "temenos" or sacred space, in which the deepest emotions, fantasies, and events can manifest themselves. Clients recreate the traumatic events in their native language, play. An underlying assumption to this treatment is that the psyche, given the opportunity, will lead the individual to wholeness and health. The centering archetype, the Self, emerges, and the ego organizes around it (Weinrib, 1983). The therapist is non-intrusive, and mirrors the child's play.
The element earth is associated with the first chakra, which is located at the base of the spine. It is associated with the life, death and survival. Food, clothing, shelter are the issues of existence on earth. Danger involving the possibility of death will trigger this chakra to open. For example, if you were crossing the street and a car were rapidly approaching, your first chakra would open wide and move you quickly out of the way.
Earth in the symbolic process is associated with grounding, nurturance, structure, consistency and survival. Its Medicine Wheel direction is North, from where wisdom and the white buffalo emerge. In astrology, earth signs are Taurus (physical existence and bounty), Virgo (service and analysis) and Capricorn (greater social structure). In Tarot, stones, pentacles or discs represent earth issues such as work, money and production.
The quality of the element is feminine and receptive. All life is sustained by the earth. It is the place of planting as well as harvest. In order to make our ideas and dreams manifest, we must bring them to the physical plane: the earth. Earth is the place of renewal. In many forms of meditation students are taught to "ground" or "anchor" into the earth through their feet or "root" chakra and instructed to pull energy up from the earth to cleanse and then release energy back into the earth where it can be transmuted into a new form. Navajo sand paintings use the element earth for curing diseases in much the same manner. The feet connect us to earth; it is where we make the human/spirit connection. The colors associated with earth are often rich greens and browns. Drumming connects us to the earth vibration, the human heartbeat to the heart of the planet. When you hear a beat or rhythm, when people start moving, making themselves real, tapping their toes, swaying; this is earth.
The feeling of earth may be warm or cold, dry or moist. We may experience earth in a tray as being a barren desert, a high mountain top, a lush garden or deep forest. Each of these scenes will elicit a different feeling in both clinician and client. The sign of earth is solid.
The developmental issue associated with earth is trust vs. basic mistrust. Being in a life-threatening situation will cause one to become ungrounded and dissociated. Psychotic and autistic clients are also earth deficient by the nature of their process being so removed from the physical plane; they are dissociated. We can attest to a different level of security that may be seen in these individuals when they are in a more natural environment. In a residential treatment center for autistic/schizophrenic adolescents, one of the programs was to be in the Mendocino woodlands for four weeks. Out of control teenagers were suddenly cooperative and calm. They were able to help with the cleansing of clothes and complete tasks much more successfully than at home. Anxiety falls away and nature fills and inspires. Remember your last walk on the beach, or hike in the woods. We know apartment dwellers who keep a bag of potting soil in the closet, taking it out to feel and smell. It's a little gesture, but it keeps them in touch with something elemental.
Earth provides structure and consistency,
a sense that the world is a predictable place. Sandplay provides both the earth
and container for therapy to exist. It is important to be able to count on a
given reaction following a particular action. How a therapist provides earth
in their work is to have a consistent predictable schedule, (i.e.,  meeting
a certain day of week, for determined number of minutes, plenty of notice before
vacations, same office) and also in being present. Earth is where therapy and
life happen. It is where change needs to manifest to have a result.
meeting
a certain day of week, for determined number of minutes, plenty of notice before
vacations, same office) and also in being present. Earth is where therapy and
life happen. It is where change needs to manifest to have a result.
Lucia, age 12, made a 3-sided pyramid emerging out of the water. On the left was land with five points protruding. After she completed the tray, she shyly and proudly said that she had her first menstruation that week. She asked me questions about my period, then at the end of the session we both went to the garden, where I gave Lucia a red rose to celebrate her becoming a woman.
Lucia unconsciously recreated the Kinaalda, the Navajo initiation ceremony for girls at the onset of puberty. The central figure in the ritual is Changing Woman who celebrated her first menstruation by "molding the earth." In this way, mountains were created.
|
Larry came for a therapy session ten days after the terrorist attack. He told me his story; being in a building one block away when the first plane hit the tower. The sounds of breaking glass, screams. He couldn't get out..a security guard blocked the exits. No one knew what was going on. The second plane hit; and someone found a TV so they witnessed the attack. He watched in horror and amazement what was occurring at the World Trade Center, only one block away. Then a huge explosion, and everything went dark. No electricity. The windows were blown out of the building. To go or stay? Larry was one of the people you couldn't see on TV, running from the dust and smoke. He was in it. He couldn't breathe. When he tells me about it, he starts to cough again, gasp for air. He can't sleep, and has been having a lot of gastrointestinal troubles since the attack. He did a sandtray:
Eleven mounds in the sand; each one contains an egg. At one end a drummer sitting within a triptych mirror, facing a rainbow and a fairy castle. On either side of the rainbow are two sequined animals; a giraffe and an elephant. In the upper left corner is a mysterious masked figure, dancing with a snake.
Larry said that the drumming in NY saved him. He was wandering around, feeling lost and disembodied. Shell-shocked. At the street corners were memorials, candles. He couldn't cry. He heard drumming, and it brought him back to his body. Since he has been home, he has been furiously drumming. I often look to where mirrors are placed in a sandtray for guidance as to my interventions. As the drummer is surrounded by mirrors, I felt that Larry needed me to mirror him on an energetic level, focusing on the rhythm of what had happened, rather than on the words. I gave him my small office drum to use after he had done the sandtray. As he drummed the pattern of horror and pain, the tears came.
The mysterious figure with the snake...who could that be? It is interesting that he is holding a snake,as the Kundalini serpent is thought to lodge in the root or earth chakra. Could this figure be holding tightly to Larry's serpent, his personal life force? The coiled serpent is the symbol of the root chakra, and this figure is holding a serpent in one hand and wear another upon his mask.
|

Maria, 35, subsequent
to the Loma Prieta earthquake. Notice the serpent under the house.
 GREENING
GREENING
Greening is a process within the
course of sandplay therapy wherein the entire tray seems to be covered in hues
of green. From deep within the dark pines, to lime-colored leaves, palms and
bushes, sparkling emeralds, waters and figures, green dominates and new growth
is heralded. It correlates to an inner season of spring and summer where new
life flourishes. This life must still be tended and nurtured to come to the
fruition and harvest. The same is true for this phase of the process in the
sand.
THE SELF
Under the earth, after the descent, archetypes of wholeness may appear.
When the ego dies, the
Self appears. The Self is the eternal center in each of us. The totality of
wholeness, the Self can never be hurt, no matter how profound the trauma or
disability an individual may face in life. Witnessing a Self tray is a deeply
moving experience. The energy in the therapy room brightens. The client and
therapist are enlivened. There is often a tingling up and down the spine that
happens in the presence of spirit, truth and new birth. The air shimmers. The
appearance of a Self tray is exactly that – a new birth. It is the new
growth from the soil, the light in the darkness. There is a union of opposites
and elements. Fire and earth, water and air often appear balanced in these trays.
Candles are often lit, mirrored objects reflecting Self appear, as well as sparkling,
luminescent figures. There is symmetry with the placement of figures creating
a mandala in the sand.
It is very important to honor this new birth as an infant, a being that needs
attention, care, nurturance and love. Be with it in that wonderful mother/infant
symbiotic state.
(The description of the Self and the elements is from Amatruda and Simpson, Sandplay,The Sacred Healing: A Guide to Symbolic Process, Trance-Sand-Dance Press: Taos, 1997.)
|
Andre, age 9, came to the sand shortly
after the war started. He made this sandplay: "This is the Americans versus the Terrorists", he said. The "terrorist" here is hardly human, perhaps a reflection of a 9 year-old's perception that what occurred on September 11 was beyond the range of his comprehension of how people treat each other.
He then wanted to create another sandpicture:
Andre looked at this silently after lighting the candles. A (young) man of few words, all he said was, "It's a meditation."
When Andre left the playroom, he was singing. The heaviness had left his body as he skipped up the stairs. He seemed to have encountered the Self, and a tiny bit of wholeness and safety was restored to his world. |
This webpage, designed by Neil Cooper, is gratefully acknowledged. It looks at the more familiar seven point chakra system from the Hindus, as opposed to the five point Tibetan chakra system used in prior discussion.
|
In India tradition
Kundalini is taught, which means coiled serpent, and refers to the energy
at the base chakra, which can under certain conditions of attunement be
made to rise like a bolt of invigorating force up the spine to the head,
through rising up the Sushuma (the middle of the three main subtle energy
channels along the spine - the others are the Ida and Pingala). This awakening
is often associated with prickly sensations on the skin or feelings of
hot and cold. Yoga students are sometime a little wary of the unpleasant
side effects if the mind is not cleansed of impurities. (source: http://www.angelfire.com/or2/spiritspeaks/chakra.html)
|
Elements in the office
While sandplay therapy is the one therapy that makes use of the actual elements (earth, water, fire and air) in a container, it is possible to have the elements accessible to your clients without a sandplay setup. One idea is to have a table near where the patient sits so that he or she can play with the figures. Things to include on the table might be:
Earth: Rocks, a 'Zen table' which is a small rectangular frame which contains sand and rocks, and comes with a small rake, plants.
Water: A small fountain, seashells, small ceramic, glass or plastic fish and sea creatures.
Fire: A votive candle, or a box of birthday candles and a bowl of sand. (Beware of the size of fire you will permit if you have a smoke alarm in the office), a figure of a small campfire. One idea is to have a floating candle, so that you have water and fire together.
Air: Feathers, a small fan, figures of birds or butterflies.

Other modalities that use cellular memory
While I have had little experience with the following therapeutic techniques, they are being used for the treatment of trauma. They are included here as they seem to access cellular memory.
Eye Movement Desensitization and Reprocessing-EMDR therapy is a "complex method of psychotherapy that integrates many of the successful elements of a range of therapeutic approaches in combination with eye movements or other forms of rhythmical stimulation in ways that stimulate the brain’s information processing system." (For more information go to http://www.emdr.com/ )
Thought Field Therapy
"Thought Field Therapy (TFT) provides a code to nature's healing system.
When applied to problems TFT addresses their fundamental causes, balancing the
body's energy system and allowing you to eliminate most negative emotions within
minutes and promote the body's own healing ability. We provide common recipes
(algorithms) or codes in our books and tapes. Specific or individual Codes are
elicited through TFT's unique assessment procedures taught in Steps A, B, and
C training programs." (source: http://www.tftrx.com/alternative_medicine.htm)
A description of how to do TFT by Charles R. Figley, PhD Psychosocial Stress Research Program and Clinical Laboratory appears at: http://www.trauma-pages.com/tft.htm
TIR or Traumatic
Incident Reduction, is a systematic method of locating, reviewing and resolving
traumatic events. Once a person has used TIR to fully and calmly view a painful
memory or chain of
related memories, life events no longer trigger it and cause distressing symptoms.
TIR has proven useful in relieving a wide range of fears, limiting beliefs,
suffering due to losses (including unresolved grief and mourning), depression,
and other PTSD symptoms. The TIR technique can be traced to roots in
psychoanalytic theory and desensitization methods; however, it is carried out
in a thoroughly person-centered, nonjudgmental and respectful context. (source:
http://www.healing-arts.org/tir/gallery.htm)
Hypnosis and Body Work also are thought to be able to assist the individual in the healing of trauma.
5. Psychopharmacology
When are medications indicated in the treatment of trauma?
Psychopharmacology of Pediatric Posttraumatic Stress Disorder By Craig L. Donnelly, M.D.
(http://www.ncptsd.org/treatment/literature/children/childpsychopharm.html) |
Recommendations for Pharmacological Treatment of Acute Stress Reactions
A National Center for
PTSD Fact Sheet
Pharmacological treatment for acute traumatic stress reactions (within one month
of the trauma) is generally reserved for individuals who already have received
individual or group debriefing and/or brief crisis oriented psychotherapy. If
these approaches are ineffective, pharmacotherapy should be considered. To date
there have been no controlled pharmacologic treatment trials for acute stress
reactions. Consequently, the present recommendations are based on controlled
studies of insomnia, anxiety and depression, as well as anecdotal experience.
Further, there are no FDA approved medications for acute stress reactions and
the only FDA approved medication for PTSD is sertraline. Prior to receiving
medication, the trauma survivor should have a thorough psychiatric and medical
examination. Ongoing medical conditions, psychiatric diagnoses, current medications
and possible drug allergies should be assessed. In addition,
questions regarding alcohol, marijuana, and other drugs should be asked since
these substances may interact with prescribed medications or may complicate
an individual’s psychological and physiological response to the trauma.
For individuals with medical and/or surgical concerns, special precautions may
be needed when prescribing psychotropic medications. Further, it is extremely
important to consider possible drug interactions in individuals who are taking
other prescribed or over-the-counter medications. In some cases psychotropic
medications may be needed even before a complete medical and psychiatric evaluation
has been completed. The acute use of medications may be necessary when the survivor
is dangerous, extremely agitated, or psychotic. In such circumstances the individual
should be taken to an emergency room. In the emergency room short-acting benzodiazepines
(e.g. lorazepam) or high potency neuroleptics (e.g. haldol) with minimal sedative,
anticholinergic and orthostatic side effects may prove effective. Atypical neuroleptics
(e.g. risperidone) also may be useful at relatively low doses in treating impulsive
aggression. After a disaster some survivors experience extreme and persistent
arousal in the form of anxiety, panic, hypervigilance, irritability and insomnia.
Empirical research has shown that hyperarousal during the first few weeks following
trauma is a risk factor for the development of PTSD. Techniques to reduce arousal
include relaxation and breathing exercises, social support, psychotherapy and
pharmacotherapy. Pharamacologic agents for the treatment of trauma-related arousal
include benzodiazepines and antiadrenergic agents such as clonidine, guanfacine
and propranolol.
Benzodiazepines are useful because they are effective and fast acting. In recent
trauma survivors, they can reduce anxiety and arousal and improve sleep. However,
prolonged use may not be indicated. In a study of trauma survivors with an acute
stress disorder (i.e. occurring 1-3 months after the trauma), the short-term
use of benzodiazepines for sleep was associated with an acute reduction in posttraumatic
stress symptoms (Mellman et al 1998). However, another study found that the
early and more prolonged use of benzodiazepines was actually associated with
a higher rate of subsequent PTSD (Gelpin et al 1996). It is recommended that
benzodiazepines be used to treat extreme arousal, insomnia and anxiety but
that their use be time limited. Other pharmacologic agents also may be helpful
in treating insomnia in persons suffering from acute traumatic stress. Low dose
trazadone, nefazodone and amitriptyline are possible choices. Antiadrenergic
agents have not been studied for the treatment of acute stress reactions, however
several open trials have been conducted in chronic PTSD. These agents have been
useful in some patients for the control of hyperarousal, irritable aggression,
intrusive memories and insomnia. Low dose propranolol also has been successfully
used for stage fright and performance anxiety because of its acute efficacy
in modulating physical and cognitive manifestations of stress. However, clonidine,
guanfacine and propranolol should be prescribed judiciously in survivors with
cardiovascular disease as they
may reduce blood pressure or, in the case of clonidine, induce rebound hypertension
if blood levels fall due to infrequent dosing or sudden discontinuation. Further,
these agents should not be prescribed to persons with diabetes as they may interfere
with counterregulatory hormone responses to hypoglycemia.
Recent trauma survivors may also suffer from debilitating symptoms of depression.
Since all three symptom clusters of PTSD respond to SSRI’s, and because
depressive symptoms originating soon after trauma may predict PTSD, it is recommended
that SSRI’s be considered for persistent post-traumatic depression. In
addition, SSRI’s may be useful to control anxiety and irritability. It
is important to note that traumatized women, compared to men, may be particularly
responsive to the beneficial effects of SSRI’s. In any case, the SSRI’s
as well as other antidepressants, should be administered in a "start low
and go slow" dosing regimen, as some individuals may develop increased
anxiety, agitation, or occasionally even psychotic or manic symptoms in response
to them. Some individuals have pre-existing psychiatric disorders at the time
that they experience trauma, including pre-existing PTSD. Trauma may exacerbate
these conditions, making careful assessment of psychotherapeutic and pharmacologic
needs essential. It is imperative that current treaters are contacted and that
continuity of care is maintained. It is also possible that trauma will precipitate
disorders other than depression, traumatic grief, acute stress disorder or
PTSD. In such cases, careful assessment and diagnosis should inform appropriate
treatment.
Finally, it is essential that treaters educate patients about potential medication
side-effects, interactions with alcohol, other medications, or substances of
abuse, and remain in close touch with patients after initiating these, as well
as other psychotropic agents. This will allow treaters to gauge the seriousness
of any side-effects, encourage compliance, and forestall untoward complications
due to extreme or otherwise idiosyncratic reactions to these medications. In
addition, the added therapeutic support can help to relieve the psychological
burden in persons suffering from posttraumatic distress.
(source: http://www.ncptsd.org/facts/disasters/fs_medication_disaster.html)
|
Janelle responded well to a change in her medication, particularly an increase in her antidepressant and an additional medication for her flashbacks. She is slowly regaining the ground she lost after the Terrorist attack. She still feels quite fragile, and in her sessions she continues to show regressed content, such as doll play, rather than the talking she had been capable of prior to September 11. She now has found the word for 'flashback' again, and has been able to communicate with the staff at the vocational center when she begins to feel overwhelmed. She is coming back, but it is still a long, long journey for Janelle.
|
|
Excerpted from:Psychopharmacology and Posttraumatic Stress Disorder by Stanley R. Platman, MD [International Journal of Emergency Mental Health, 1999, 3, 195-199.] Posttraumatic stress disorder
may develop after Clearly, more research is required
before we can Psychopharmacologic Considerations
in the
published by International Critical Incident Stress Foundation, Inc. http://www.icisf.org/Acrobat%20Documents/TerrorismIncident/PTSDPsychoPharm.PDF
|
6. Spirit
Future Action on a Personal and Community Level
Sometimes the most crucial part of changing the world is changing ourselves; bringing shadow material to consciousness, and pulling back projections. As we educate ourselves, racial and religious stereotyping diminish. After the September 11 bombing, many realized how little they knew of Islam, or the Middle East. We are learning how far away Osama bin Laden and the Taliban are from the tenets of Islam. We need though, as a culture, to understand the fear and disempowerment, the rage and pain that feeds terrorist acts. Not to excuse them, but to do what we can to prevent future generations of terrorists. No nation is exempt from terrorism.
Consciousness and compassion are the keys. Search always for the light in the darkness.
Contributions of time and energy are also important. In this course, there have been references to:
The American Red Cross
needs volunteers, and will provide training. If you can, give blood. Go to:
http://www.redcross.org/donate/volunteer/
for more information.
The Green Cross Projects (GCP) is a humanitarian service organization originally
started by the Traumatology Institute in response to the Oklahoma City bombing
in 1995. The goal of GCP is to provide immediate trauma intervention to all
areas of our world when a crisis occurs. This includes assistance in the most
recent world disaster, the issue of violence in the media, the crisis in Kosovo
and discussions on other events, such as the rampage tragedy in Littleton, Colorado
(USA). For the most recent information, other than this web site, members are
urged to read the most recent issue of the e-journal,
TRAUMATOLOGYe and the Newsletter. http://www.greencross.org/
The Association for the Study of Dreams has established a Nightmare Hot Line : They need volunteers to staff the line. Please go to: http://www.asdreams.org/nightmare_hotline.htm to help.
Education
In the West, we need to educate ourselves and our children about other cultures and religions. A good place to start is Understanding Islam, Beliefnet's Islam Primer, at http://www.Beliefnet.com/index/index_40118.html. According to this site,
"The word Islam derives from two Arabic words that point directly to the central
tenets of the faith: first, the word "taslim," which means submission; and then
the word "salam" which means peace. At the very core of Islam is submission
to God and the call to peace.
The prophet Muhammad ordered his fellow Muslims to salute all people –
fellow Muslims and non-Muslims alike – with peace. The traditional salutation
in Islam is: "Al Salamu Alaikum" – "Peace on You."
Compassion Fatigue
|
"All
strong souls first go to hell before they do the healing of the world
they came here for. If we are lucky, we return to help those still trapped
below."
- Dr. Clarissa Pinkola Estes |
|
Cora came to therapy looking exhausted. She is a therapist with a huge caseload, including children, adolescents and adults. Her task is complicated by the paperwork required by the many managed care panels on which she serves. Her pallor was gray, she had dark circles under his eyes. "I don't know how much more of this I can hear. I feel like a sponge that is saturated, there is no way to wring it out. I am carrying so much pain right now. And I don't even want to talk about it, because I don't want to burden you as well. I know that you work with children as well as adults, and I think that you're probably all filled up too." I reassured her that she could talk about how much she was carrying, but also felt that she needed us to speak as peers, as well as patient to therapist. We spoke of the horror, and how much we were holding for ourselves, our families, and our patients. She went on to add, "I also feel that we are doing this for the country and the world as well. That therapists somehow hold the heart and soul of the people, and we have to feel all the feelings." Cora is probably unconsciously doing the Tonglen Meditation, or The Seven Points of Mind Training Exchanging Self for Others. "The core practice involves taking on others' sorrow and pain and sending them your joy; not as a masochistic practice but with the aim of getting away from the self-centeredness and self-seeking that cause us so much pain. These practices were brought to Tibet in the eleventh century by the Indian Buddhist teacher Atisha." For more on this, please go to: http://www.theflow.org/tonglen/
|
Compassion Fatigue is when we are tired, and have no more room for compassion. Perhaps we are overwhelmed, or filled up, with all the stories and all the pain. Compassion fatigue doesn't only happen to therapists; doctors, ministers, EMTs, all those in the 'Helping Professions' can reach the point at which there is no more help to give. Caretakers also can suffer from this; a parent with a disabled child, a spouse taking care of a partner with Alzheimer's, a person whose partner has a chronic or terminal illness can all get to the place of being empty.
The term Compassion
Fatigue, coined by Dr. Charles Figley of Florida State University, is defined
as "a condition common to professional care-givers that is described as
a union of secondary
traumatic stress and burnout. Secondary trauma occurs when one is exposed to
extreme events that were directly experienced by another person. Burnout is
a state of physical, emotional and mental exhaustion caused by an overwhelming
depletion of ability to cope with one's everyday environment. (source: http://www.psychink.com/press.html)
There is a copy of the
Compassion Satisfaction and Fatigue (CSF) Test, written by B. Hudnall
Stamm & Charles R. Figley at: http://www.isu.edu/~bhstamm/satfat.htm
There is a concept called Vicarious Traumatization or VT. "Vicarious traumatisation refers to the cumulative transformative effect upon the trauma therapist of working with survivors of traumatic life events. .... It is a process through which the therapist's inner experience is negatively transformed through empathic engagement with clients' trauma material" http://www.massey.ac.nz/~trauma/issues/1998-2/steed.htm
In Professionals Coping with Vicarious Trauma Josef Ruzek, Ph.D. in the NCP Clinical Newsletter 3(2): Spring 1993 quotes J. L. Herman(1992. Trauma and Recovery. U. S. A.: Basic Books):
"Engagement in this work thus poses some risk to the therapist's own
psychological health. The therapist's adverse reactions, unless
understood and contained, also predictably lead to disruptions in the
therapeutic alliance with patients and to conflict with professional
colleagues. Therapists who work with traumatized people require an
ongoing support system to deal with these intense reactions. Just as no
survivor can recover alone, no therapist can work with trauma alone".
http://www.ncptsd.org/treatment/cq/v3/n2/ruzek.html
What we can do
Kuan Yin
(source: http://www.tbsn.org/english/library/sutras/kuanyin.htm)
A helpful meditation is to give all your pain, and that of your clients, and that of the the world, to Quan Yin.
The lines from T.S. Eliot's Four Quartets "Oh dark dark dark" keep running through my brain, as I contemplate what is happening to the world.
I begin my own process of grief. I ask for the help of Kuan Yin, the Bodhisattva of Compassion, to help me hold the pain and grief. Her name means "She Who Hearkens to the Cries of the World". She is also known as Quan Yin, Kannon, Avalokitesvara, Miao Shan and Tara.
Here she is depicted with
a bottle, pouring out her endless compassion and mercy on us all. (For more
images of Kuan Yin, please go to ![]() Kuan
Yin.) One story of Kuan Yin states that she was on the threshold of Nirvana
when she heard the cries of human pain. She (or He; Kuan Yin is sometimes referred
to as male) stopped and would not cross. She will stay with us until all the
tears have been shed.
Kuan
Yin.) One story of Kuan Yin states that she was on the threshold of Nirvana
when she heard the cries of human pain. She (or He; Kuan Yin is sometimes referred
to as male) stopped and would not cross. She will stay with us until all the
tears have been shed.
Quan Yin is one of the most universally beloved of deities in the Buddhist tradition. Also known as Kuan Yin, Quan'Am (Vietnam), Kannon (Japan), and Kanin (Bali), She is the embodiment of compassionate loving kindness. As the Bodhisattva of Compassion, She hears the cries of all beings. Quan Yin enjoys a strong resonance with the Christian Mary, the Mother of Jesus, and the Tibetan goddess Tara.
In many images She is depicted carrying the pearls of illumination. Often Quan Yin is shown pouring a stream of healing water, the "Water of Life," from a small vase. With this water devotees and all living things are blessed with physical and spiritual peace. She holds a sheaf of ripe rice or a bowl of rice seed as a metaphor for fertility and sustenance. The dragon, an ancient symbol for high spirituality, wisdom, strength, and divine powers of transformation, is a common motif found in combination with the Goddess of Mercy. Sometimes Kuan Yin is represented as a many armed figure, with each hand either containing a different cosmic symbol or expressing a specific ritual position, or mudra. This characterizes the Goddess as the source and sustenance of all things. Her cupped hands often form the Yoni Mudra, symbolizing the womb as the door for entry to this world through the universal female principle. Quan Yin, as a true Enlightened One, or Bodhisattva, vowed to remain in the earthly realms and not enter the heavenly worlds until all other living things have completed their own enlightenment and thus become liberated from the pain-filled cycle of birth, death, and rebirth.(source: http://www.crystalinks.com/quanyin.html)
Tikkun Olam
In the Kabbalah, an
ancient Jewish mystical text, is the concept of 'tikkun olam'. "The true
self within
something is referred to in Kabbalah as a holy spark, and the Zohar tells us
that nothing can exist without having a spark of holiness at its core. The process
of removing barriers to release these sparks is known as tikkun, correction
or repairing. To repair the world at large through good works is tikkun olam,
and to repair one's individual soul is tikkun nefesh. " (source: http://web.wt.net/~cbenton/kabbalah/klippot.htm)
Thich Nhat Hanh
Buddhist teacher Thich Nhat Hanh, quoted in Buddhist teachers with Berkeley ties counsel pacifism by Don Lattin (S.F. Chronicle, 10/14/01) was asked what he'd say if he could speak to Osama bin Laden.
"The first thing I would do is listen," he replied,
"listening with great will to understand the roots
of suffering that are the cause of the violent
action."
Does he favor a military strike against the
terrorists or the nation's that are harboring them?
No.
"All violence is injustice," he said. "The fire of
hatred and violence cannot be extinguished by
adding more hatred and violence to the fire. The
only antidote to violence is compassion."
Then what would he do?
"We have to find a way to stop violence, of
course. If need be, we have to put the men
responsible in prison."
Why is this happening to America? Why do they
hate us?
"The deep reason for our current situation is our
patterns of consumption. U.S.A. citizens
consume 60 percent of the world's energy
resources yet they account for only 6 percent of
the total world's population."
(source: http://www.sfgate.com/cgi-bin/article.cgi?file=/chronicle/archive/2001/10/14/LV223812.DTL)
Chögyam Trungpa
There is a moving article entitled "The Four Foundations of Mindfulness Meditation" by Chögyam Trungpa. Included are discussions and practices for Mindfulness of Body, Mindfulness of Life, Mindfulness of Effort and Mindfulness of Mind. This article is at http://www.shambhala.org/teachers/vctr/fourfoundations.html
Your own spiritual practice
Whether you are Jewish, Christian, Islamic, Buddhist, Pagan, or ????, now is a good time to revive your spiritual practice, be it praying, walking in the woods, meditating, etc. Anything that allows us to feel connected to some force who is greater than ourselves, and who will help us hold the pain, is a good thing right now.
Stop and take breaks. Turn off the TV and the radio. Exercise, Take your vitamins and try to eat healthy food. (Yes, Mom). Reread your favorite books from childhood. Surround yourself with beauty. Go for walks. Kiss and hug your family and friends. Drink really good coffee and tea. Keep a journal. Doodle. Laugh. Practice 'random acts of kindness and senseless acts of beauty'. Cry when you feel like crying. Dance. Wear your favorite clothes, so you look like a million dollars (even if you don't feel like a million dollars). Honor your shadow, by acknowledging some really horrible part of yourself that it is easier to project onto someone else...this work can save the planet, if everybody did it. Speak out against racial and religious stereotyping. Honor your heroes. Listen to Louis Armstrong singing, "What a Wonderful World."
One meditation that helps me is adapted from the Tibetan Book of the Dead. What I try to do every night as I fall asleep is to remember:
one beautiful sight from the day...
a sound that gave me pleasure (could be music, or bird song, or my partner saying, "I love you")...
a delicious taste...
a wonderful smell...
a soothing touch...
One pleasing memory for each sense, to help me appreciate being on this little planet.

Suzanna, age 9
Hope
It is important to remember and reaffirm the healing power of the human spirit, and the resiliency of the heart. Please try to not lose hope as you do this crucial work. Healing is possible. There is a part in each of us, called by different names: the Self, the soul, the spirit, the being...that can never be harmed or injured, no matter what has happened to the body or psyche of the person traumatized. If we as healers can hold onto this light, even in the darkest times, then healing is not only possible, it is probable.
Go well in your journey as a healer.

We do adhere to the American Psychological Association's Ethical Principles of Psychologists. Our courses are carefully screened by the Planning Committee to adhere to APA standards. We also require authors who compose Internet courses specifically for us follow APA ethical standards. Many of our courses contain case material, and may use the methods of qualitative research and analysis, in-depth interviews and ethnographic studies. The psychotherapeutic techniques depicted may include play therapy, sandplay therapy, dream analysis, drawing analysis, client and therapist self-report, etc. The materials presented may be considered non-traditional and may be controversial, and may not have widespread endorsement within the profession. www.psychceu.com maintains responsibility for the program and its content. |
|
Thank
you for joining us in this class! |
888-777-3773
|
|


 Josh
is eight. His anxiety a few weeks after the bombing was still quite high.
School was stressful, he was having a hard time concentrating. His processing
of the bombing was complicated by a sudden, serious illness of a very
close family friend. Josh was not feeling very safe in the world. He made
a huge volcano for his sandtray, perhaps expressing how worried his heart
was, how disempowered he felt, and his anger at what had happened to his
world.
Josh
is eight. His anxiety a few weeks after the bombing was still quite high.
School was stressful, he was having a hard time concentrating. His processing
of the bombing was complicated by a sudden, serious illness of a very
close family friend. Josh was not feeling very safe in the world. He made
a huge volcano for his sandtray, perhaps expressing how worried his heart
was, how disempowered he felt, and his anger at what had happened to his
world.