|

Learning about Current Programs of Recovery and How Therapists Can Effectively Utilize These Programs
As you will see throughout
the links there are a wide variety of treatment programs available to an individual
who has accepted that addiction is a problem .
In order to determine the
appropriate program for your client there are many considerations. For specific
questions or populations, go to ![]() Understanding
Substance Abuse Prevention: Toward the 21st Century: A Primer on Effective
Programs http://www.samhsa.gov/centers/csap/modelprograms/pdfs/monograph.pdf
Understanding
Substance Abuse Prevention: Toward the 21st Century: A Primer on Effective
Programs http://www.samhsa.gov/centers/csap/modelprograms/pdfs/monograph.pdf
http://www.niaaa.nih.gov/publications/niaaa-guide/index.htm
Alcohol Problems
|
 |
As a marriage and family therapist, you are likely to see many individuals, couples, and families in your practice who are experiencing or are at risk of experiencing significant alcohol-related problems. This Guide will:
AN ALCOHOL PROBLEMS FRAMEWORK
Since the 1930s, "alcoholics" — have been the primary focus of alcohol-related
intervention efforts in the United States. While a focus on severe problems
is typical of an initial societal response to a health problem,1 alcohol
dependence represents only a small portion of the entire range of alcohol-related
problems.2 Most drinking problems are of mild
to moderate severity3 and are amenable to relatively
brief interventions. In a report to the National Institute on Alcohol Abuse
and Alcoholism (NIAAA), the Institute of Medicine (IOM)4 called
for a "broadening of the base for treatment" and widespread adoption of an
alcohol problems framework. This framework casts a wide net for treatment efforts,
explicitly targeting individuals (or families) who currently are experiencing
or are at risk for experiencing alcohol problems. Thus, therapists and health
care professionals are asked to direct interventions not only to drinkers with
alcohol use disorders, but also to problem drinkers and "at-risk" drinkers.
Alcohol Use Disorders
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition5 (DSM-IV)
recognizes two alcohol use disorders: alcohol dependence and alcohol abuse.
Problem Drinking and Risky Drinking
As it is commonly used, "problem drinking" often is synonymous with "alcoholism." Among
professionals, however, increasingly it is used to describe nondependent drinking
that results in adverse consequences for the drinker.6 In
contrast to the dependent drinker, the problem drinker's alcohol problems do
not stem from compulsive alcohol seeking, but often are the direct result of
intoxication. Problem drinking represents a broader category than alcohol abuse
disorder. The problem drinker may or may not have a problem severe enough to
meet criteria for alcohol abuse disorder.
| Even small amounts of alcohol consumed during pregnancy or in combined with certain medications may result in significant adverse consequences and therefore constitute risky drinking. |
While problem drinkers are currently experiencing adverse consequences as a result of drinking, risky drinkers consume alcohol in a pattern that puts them at risk for these adverse consequences. Risky drinking patterns include high-volume drinking, high-quantity consumption on any given day, and even any consumption, if various medical or situational factors are present. Consumption is quantified in terms of standard drinks, which contain approximately 14 grams, or .6 fluid ounces, of pure alcohol (See Appendix B for a graphic portraying standard drink equivalencies for popular alcoholic beverages). Risky drinking can be determined by identifying one or more of the patterns below:
 d d |
THE CONTINUUM OF ALCOHOL PROBLEMS
Alcohol problems can range in severity from mild, negative consequences in
a single life situation to severe alcohol dependence with significant medical,
employment, and interpersonal consequences. As shown in Figure 1, alcohol
use and its associated problems can be viewed on a continuum — ranging
from no alcohol problems following modest consumption, to severe problems
often associated with heavy consumption.
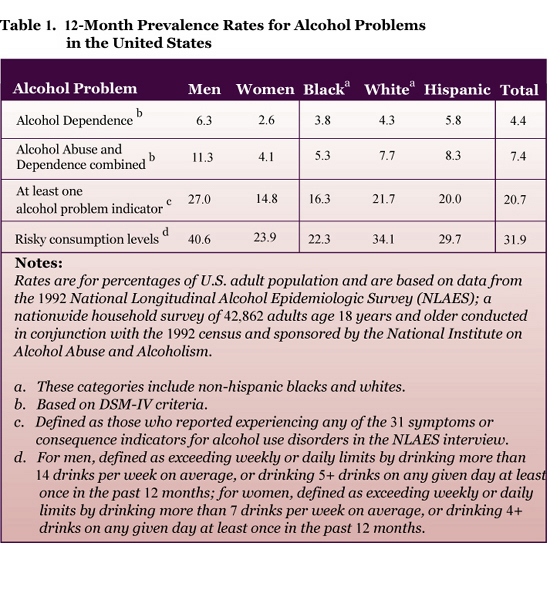
THE PREVALENCE OF PROBLEMS
Alcohol abuse and alcohol dependence are among the most prevalent mental disorders
in the United States.7 In 1992, 7.4% of U.S.
adults aged 18 years and older — roughly 14 million Americans — were
found to have an alcohol use disorder (alcohol dependence or abuse).8 (See
Table 1.)
 d d |
Population estimates for alcohol use disorders do not include the millions of adults who experience less severe alcohol-related problems or who engage in risky drinking patterns that could potentially lead to problems. Criteria for alcohol use disorders are relatively clear, but establishing a "cut-off point" to separate problem drinkers from nonproblem drinkers is difficult, making population estimates more problematic.9 Although a pattern of recurrent trouble related to alcohol may indicate a more serious alcohol problem, experiencing any alcohol-related problem is cause for concern.10 As shown in Table 1, a recent national study found that approximately 21% of Americans experienced at least one alcohol-related problem in the prior year, and roughly 1 in 3 Americans engaged in risky drinking patterns.
These base rates for alcohol problems and risky drinking are high in the general population, but they are considerably higher in clinical populations. Given the high rates of co-morbidity between alcohol use disorders and other psychiatric disorders, and the strong association that exists between drinking behavior and mood regulation, stress, and interpersonal and family problems, a high proportion of individuals, couples, and families who present for therapy may be experiencing or may be at risk for alcohol problems.
ALCOHOL PROBLEMS: THE COUPLE AND FAMILY
CONTEXT
When someone experiences alcohol problems, the negative effects of drinking
exert a toll, not only on the drinker, but also on their partner and other
family members.11 Recent data suggest that
approximately one child in every four (28.6%) in the United States is exposed
to alcohol abuse or dependence in the family.12
One of the clearest demonstrations of how alcohol use negatively impacts the family is the widely documented association between alcohol use and interpersonal violence.13 Family problems that are likely to co-occur with alcohol problems include:14
IMPLICATIONS FOR INTERVENTION
The alcohol problems framework explicitly recognizes tremendous heterogeneity
in the severity, duration, progression, etiology, consequences, and manifestations
of alcohol problems. If you wish to address alcohol problems in your individual,
marital, or family practice, this heterogeneity requires that you are equipped
with:
| Epidemiological data confirm the well-known discrepancy in rates of alcohol problems for men and women. Men are nearly three times more likely than women to have alcohol use disorders and about twice as likely to experience mild to moderate alcohol problems and to engage in risky drinking. However, women have higher rates of morbidity and mortality from alcoholism than men. |
The tools we recommend for screening and assessment are flexible enough to be used with adults in individual, couple, or family therapy contexts. At times, you will be required to screen and assess alcohol use in adolescents, but such assessments are beyond the scope of this Guide. For information on the assessment and diagnosis of alcohol use disorders in adolescents, see www.niaaa.nih.gov/publications/arh22-2/95-106.pdf.
Appendix A features copies of exemplary instruments for both screening and problem assessment, creating a complete "Clinical Toolbox" for you to use in your practice.
SCREENING FOR ALCOHOL PROBLEMS
The objectives of a brief screen are to:
If an individual presents for therapy with a self-identified alcohol problem, it is prudent to skip the screening step and move directly to further assessment of the alcohol problem. However, screening should be conducted routinely with other presenting adult family members (e.g., the spouse). Even in the context of individual therapy, it is useful to routinely gather information from the client about the alcohol use of their spouse or other adult family members who are not present to determine whether a family member's drinking may be contributing to the client's problems.
Screening Instruments
A number of standardized screening instruments are available to help you quickly
identify current and potential alcohol problems. These brief screening tools
are designed to identify as many potential cases as possible, while at the
same time minimizing false positives. Recommended tools include:
The instruments can be either self-administered, for clients who have sufficient reading ability, or used in a face-to-face structured interview format. Based on the presenting problem, time constraints, family constellation, and other factors, you will need to determine whether the screening protocol is most effectively delivered in an interview format during the session, or whether it would be more effective to have individual family members complete paper or computer-assisted assessments. The interview format allows you to probe further and reconcile inconsistencies, but it may not be an efficient use of limited session time — especially when multiple family members need to be assessed.
ALCOHOL PROBLEM ASSESSMENT
Screening for alcohol problems should be considered only a first step. Screening
alone does not provide enough information to make either a diagnosis or an
informed treatment decision. If an individual or family screens positive,
i.e. there are indications of risk, further assessment is required to confirm
the problem and to determine its nature, extent, and severity.
Since screening instruments are designed to err on the side of inclusion, (i.e., to maximize sensitivity rather than specificity), the initial goal of a more intensive problem assessment is to confirm or rule out the presence of an alcohol problem.
Primary goals of the problem assessment are to:
Although our overview is limited to a review of assessment strategies and instruments related specifically to alcohol problems, a broader assessment that covers other areas of psychological and interpersonal functioning is recommended prior to clinical intervention. Clinician skill and preference, as well as client literacy, will determine whether self-report instruments or interviews are selected.
Level and Pattern of Alcohol Use
Self-reports of the frequency and quantity of recent alcohol use remain the
most reliable indicators of alcohol consumption patterns available. However,
if the person is intoxicated at the time of assessment or has a severe drinking
problem, consumption measures may not be accurate25 and
should be corroborated with other markers of drinking behavior, such as biomedical
markers or collateral (e.g., a spouse) reports.26 There
are three major types of methods for assessing consumption, each of which
has particular strengths and weaknesses:
Dependence Symptoms and Severity of the
Problem
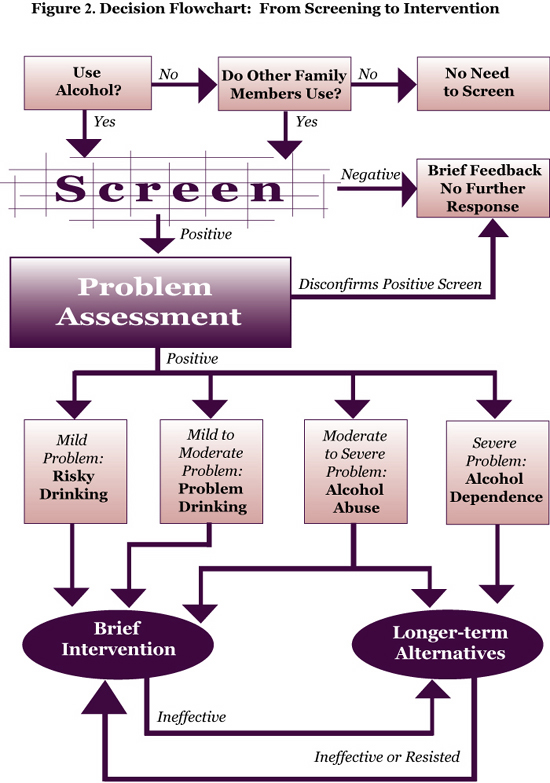
Assessing dependence symptoms is critical to determining the appropriate treatment
option (See Figure 2 - Decision Flowchart: From Screening to Intervention).
Two validated self-report instruments are:
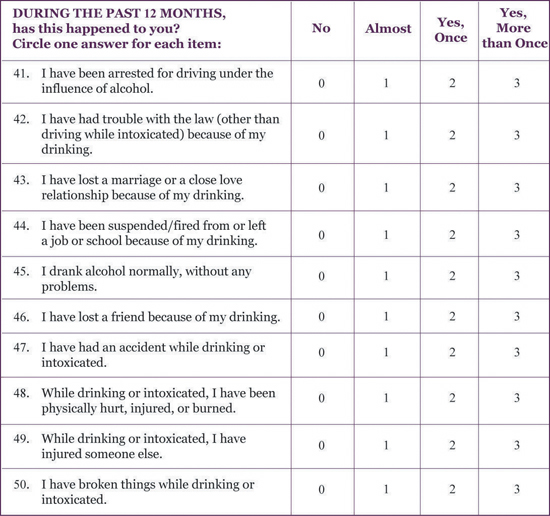
Consequences of Alcohol Use
Drinking consequences represent a domain independent of dependence symptoms
and should be measured separately. While many screening instruments and diagnostic
clinical interviews contain interview questions designed to identify negative
consequences, having your clients complete a self-administered questionnaire
will provide a detailed picture of negative consequences across a variety
of life domains, and in the case of marital or family assessment, from different
family member perspectives.
A thorough assessment of consequences also can be useful when evaluating treatment effects, since these measures have been shown to be sensitive to changes in drinking-related problems over time.31 Communicating these assessment results often is useful in helping the drinker appreciate the connection between drinking and negative consequences across life domains.
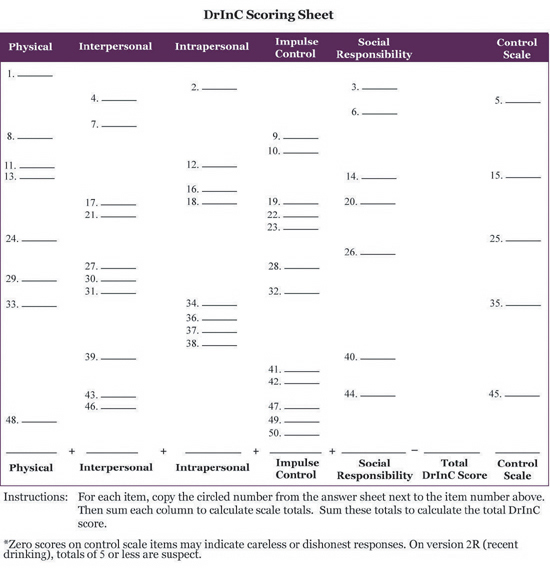
The Drinker Inventory of Consequences32 (DrInC) is a 50-item checklist of potentially adverse drinking consequences that provides summary scores in five areas:
FROM SCREENING AND ASSESSMENT
TO DECISIONS AND ACTION
Figure 2 summarizes the process of screening and problem assessment that we
have described thus far. The next step in the process is to choose an intervention
strategy that matches the nature of the identified problem.
By broadening the target population for alcohol-related interventions
to include people with risky drinking patterns and mild to moderate alcohol
problems, you will address a wider range of concerns that families may
have about drinking. The goal of treatment also is necessarily broadened.
From an alcohol problems framework, the overall goal of treatment is "To
reduce or eliminate the use of alcohol as a contributing factor to physical,
psychological, and social dysfunction and to arrest, retard, or reverse
the progress of associated problems." 33
 d d |
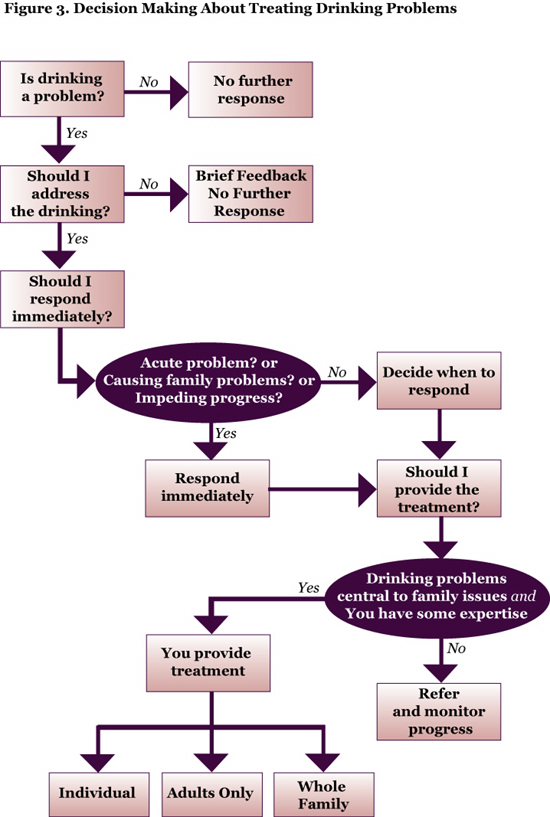
Once you have identified an alcohol problem and have determined that a brief intervention approach would be appropriate, you are faced with a series of clinical decisions. The next sections of this Guide will walk you through the steps required to achieve a successful response from an individual, couple, or family client with an identified alcohol problem.
Once you become aware that drinking is a problem for a family, you must ask yourself a series of questions:
 d d |
Determine the Type and Severity of the
Alcohol Problem
Family alcohol problems can range in severity from conflicts about what is
considered acceptable drinking behavior to severe alcohol dependence with resulting
physical dependence or medical problems.35 More
severe problems will require immediate, specialized attention; those that are
less severe can be addressed in the context of the overall treatment plan.
Decide Whether Identified Drinking Problems
Should Be Addressed
Although it might seem counter-intuitive to ignore an important problem, there
may be reasons for doing so:
Decide on the Timing of Your Response
Decide Whether to Treat Alcohol Problems
Within Family Treatment or Through Referral
At least two elements will contribute to this decision:
Decide Whether to See the Entire Family
or Just the Drinker
If drinking is central to a family's problems, and you decide to intervene,
it may be necessary to put aside other aspects of the family therapy until
the drinking problem is stabilized and changes have been initiated. You may
see the individual family member with the identified drinking problem alone
for a period of time, and then bring other family members back into treatment.
Decide Whether to Involve the Children
There are several positive reasons for involving the children:
Involving children in treatment sessions may also present drawbacks:
RAISING DRINKING ISSUES IN THE
CONTEXT OF FAMILY THERAPY
There are no simple answers to the clinical decisions outlined above. If you
decide to bring drinking problems into the therapeutic agenda, the next challenge
is to determine how you can raise drinking issues and facilitate the family's
acceptance of drinking as a legitimate part of the therapeutic agenda.
This section provides two vehicles for broaching the initial discussion of alcohol problems — linking drinking to presenting family concerns or linking drinking problems to problems encountered in progressing toward therapeutic goals.
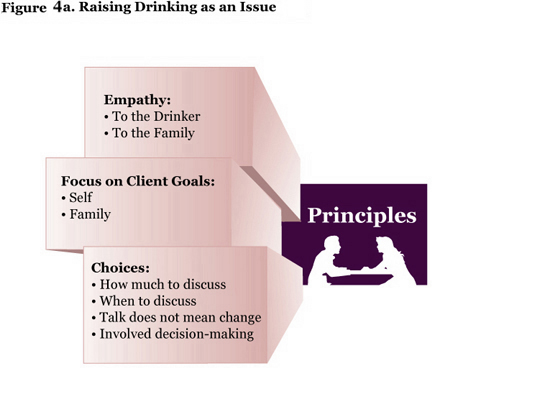
The use of three major therapeutic principles — empathy, motivation
through attention to client goals, and choice — can facilitate
the successful introduction of drinking issues into therapy. Figures
4a and 4b identify the key principles and pitfalls to consider when addressing
drinking as an issue in family treatment.
 d d |
 d d |
SOME GENERAL THERAPEUTIC PRINCIPLES
Accurate Empathy is Strongly Associated
With a Positive Response to Treatment for Drinking Problems
Traditional approaches to alcohol treatment have taken a more confrontational
style in which attempts are made to "break through" client denial to facilitate
awareness of the extent and severity of their drinking. Research, however,
does not support this approach. Instead, it finds that clinicians who can understand
the complex emotions clients experience concerning his/her drinking and who
can communicate this understanding in an empathic and supportive manner are
more likely to achieve success in enabling clients to: (1) discuss their drinking,
(2) realize the problems associated with it, and (3) prepare to change. From
the first moment that you address drinking, utilizing an empathic approach
is crucial.
Enhance Motivation by Focusing on Client
Goals
Traditional views of change in drinking habits held that motivation was a trait
that a client either did or did not have. Life experience, not clinician or
family action, was the vehicle by which motivation would lead to change. However,
contemporary research contradicts this traditional view. It offers substantial
evidence that you can enhance your clients' motivation to change by using specific
therapeutic behaviors, and by providing family members with interventions to
change their behavior as well. (See Elements of Brief Interventions: When
the Drinker is Not Present, page 35).
You can enhance client motivation by linking the client's drinking to their own positive goals. In particular, if there is a discrepancy between the client's current life circumstance and the specific goals that he/she has articulated, drinking may be contributing to this discrepancy between goals and desires. Helping the client make this linkage can provide a powerful source of motivation to change.
Give Client Choices
Providing clients who have drinking problems with choices about how to select
treatment options and how to articulate treatment goals will result in better
treatment retention and more positive outcomes. Instead of assuming an authoritative
stance that directs the drinker to one course of action, you can provide
choices that help the drinker to become knowledgeable about these options.
You also can provide guidance about the advantages and disadvantages of various
options without trying to force the client to select a specific choice.
APPLYING THE GENERAL PRINCIPLES
How can you use the three principles to successfully introduce drinking issues
into family therapy?
Any Discussion of Drinking Should Be Approached
With An Empathic and Respectful Demeanor
You might introduce the topic by saying:
Link Drinking to Client Goals and Aspirations
In family therapy, applying this principle is relatively easy. Clients seeking
family therapy typically have a set of concerns that motivated them to seek
assistance:
Noncompliance with homework assignments, observing that specific types of assignments fall apart (e.g., having a couple go out together, or discuss a problem during the evening), or feeling bewildered about aspects of a family's functioning, are all clues that the drinking might be a contributing factor. Feedback about the linkages between drinking and lack of progress in treatment also can be used to introduce the topic of alcohol into therapy.
Applying Principles of Choice
The principle of "choice" becomes prominent as alcohol issues are explored
more fully, but even in the initial discussion, you must keep this principle
in mind. After first discussing drinking, you can give the family a choice
about the degree to which the topic is pursued in any one session. You also
can be clear that discussing drinking is not equivalent to requiring that anyone
change their behavior, and that the family will be involved actively in decision-making
about how to proceed.
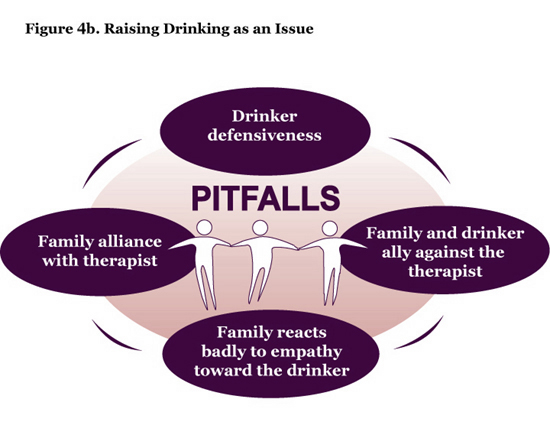
SOME COMMON PITFALLS
Although this Guide assumes that it ultimately will be constructive and valuable
to address drinking in the context of marital or family therapy, you must
be prepared for pitfalls that are unique to the marital/family therapy context:
Defensiveness On the Part of the Drinker
Expect to hear assertions that the drinking is not a problem, is under control,
can be controlled whenever the drinker desires, or that others are "making
too big a deal about a few drinks." The three therapeutic principles that
guide this section — empathy, motivation through goals, and choices — are
all intended to attenuate the drinker's defensive reactions.
Reactions of Other Family Members During
Any Discussion of Drinking
Family members may experience relief that the topic is being addressed, and
may make strong efforts to ally with you against the family member with the
problem drinking.
Such comments as, "I've been concerned about that too," or "She's right, we have to face this," are hints that a family member is trying to become your ally against the drinker. You must make efforts to neutralize the alliance, i.e., maintain an alliance with the family as a unit, rather than with specific family members.
Negative Reactions by Family Members to
Your Empathic Responses to the Drinker
Family members, who often have experienced anger, frustration, fear, and sadness
in response to years of problem drinking, may be impatient to see change occur
once the topic of drinking is introduced into therapy. They may hope that you
will "straighten out" the drinker, providing definitive instructions to stop
the drinking behavior and to seek a specific form of treatment. When you do
not respond accordingly, family members may react negatively. They may become
angry with you for expressing empathy about how difficult it is to face and
change a drinking problem, or for trying to help the client make decisions
about how, when, and how much to change. You must walk a careful line, not
sacrificing the needs or desires of any family member to those of others in
the family. A balanced, empathic, and respectful response to the reactions
of each family member can neutralize some of the intense emotions that surround
this topic.
Family Members May Develop Alliance Against
You
As a reflection of their desire to avoid discussing the role of alcohol in
their family or the problems it has caused, the family may develop an alliance
against you. Different factors may lead to a family alliance to avoid any discussion
of drinking, including:
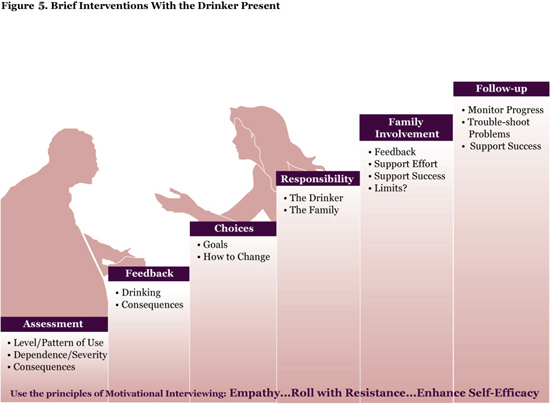
Major elements of the brief intervention include:
 d d |
GENERAL THERAPEUTIC APPROACH — USE
OF MOTIVATIONAL INTERVIEWING STYLE
Motivational interviewing is an empathetic, client-centered, therapeutic style
and should be used when conducting brief interventions. Three major principles
underpin motivational interviewing:38
Express Empathy
Empathy implies an acceptance of each family member's experience, perspectives,
and emotions, and requires the ability to express this acceptance in a warm,
compassionate manner. The use of active reflective listening is key.
Roll With Resistance
Drinkers often attempt to persuade others that their drinking is not problematic.
Such an argument tends to solidify the drinker's viewpoint. If you avoid
arguments, empathically accept that the drinker is ambivalent, and encourage
the drinker to merely consider an alternative viewpoint, resistance is likely
to decrease.
Enhance and Support Self-efficacy
You should view the drinker as capable of changing and communicate that perspective
in a number of ways:
ASSESSMENT
For the brief intervention, you should obtain information that will help the
drinker and other family members understand why and in what ways their drinking
is problematic. Several types of information, which can be obtained using
questionnaires and interview questions, are helpful in achieving this understanding
(See Alcohol Problem Assessment, page 8).
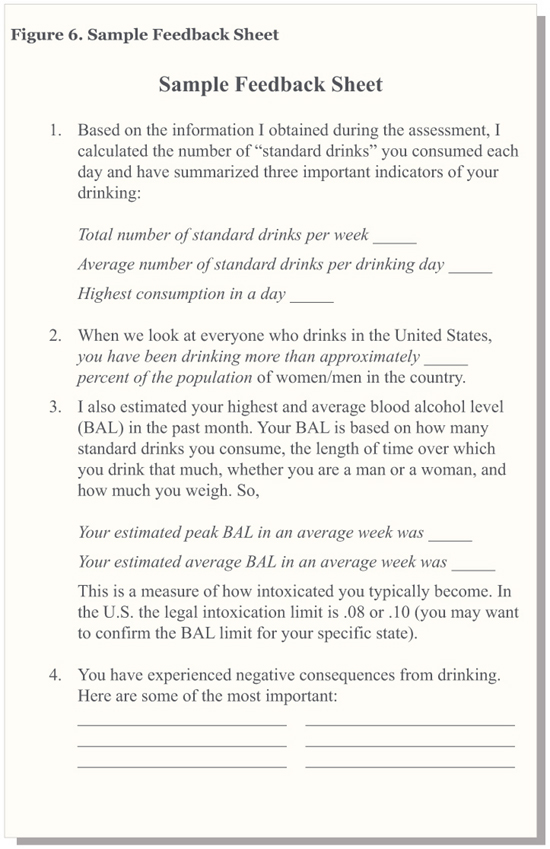
FEEDBACK
A key element in brief interventions is the feedback provided to the drinker.
A major purpose of feedback is to help the drinker recognize discrepancies
that exist between his/her current circumstances and personal and family
goals and aspirations. Feedback should be conveyed in a warm, empathic tone,
and should be descriptive rather than evaluative. The clinician may introduce
the feedback by saying:
Feedback About Drinking
 d d |
 d d |
 d d |
Feedback About Negative Consequences of
Drinking
Information about negative consequences has been provided already by the drinker
and other family members, but summarizing negative consequences often has a
notable impact. The clinician can organize this section into:
After the Feedback
At the conclusion of the feedback session, client and family reactions will
vary widely:
CHOICE
After discussing reactions of the drinker and family members to the feedback,
the conversation should move to determining possible next steps. Here, it
is important to ensure that the drinker has choices and does not feel forced
to select one option. Any movement toward change should be considered a positive
outcome of the brief intervention. Although total abstinence from alcohol
is always a safe, desirable outcome, reductions in drinking can lead to improved
health and social functioning. Reductions in drinking also may serve as a
way station to abstinence, whereby the drinker attempts to cut down, and
ultimately decides that abstinence is either an easier choice or a necessary
one. Although some drinkers may ask for specific advice and information about
available treatments, many may respond by stating that they accept the need
for change but want to try to change on their own. Both treatment and self-change
can lead to positive results, so you can support either plan.
Providing a drinker with choices is more than passive acceptance of the individual's goals and preferred route to change. You can play an active role by providing specific information about different goals and different treatment options. Lay out your view of the advantages and disadvantages of each option, and even suggest a preferred course of action. Having an educational discussion and clearly stating the importance of choosing a route to change that is acceptable will enhance the likelihood of success.
Although the main target of this discussion is the drinker, the other family members should be encouraged to express their views about advantages and disadvantages of different approaches. By the end of the discussion, the ideal outcome invokes a specific change plan. Referral for specialty treatment; involvement with self-help; continued work on the drinking in the family therapy; or an initial attempt at self-change are all acceptable change plans. If the drinker is not willing to commit to any plan, you should respect that choice, but indicate that you will return to a discussion of drinking in future sessions after the entire family has had the opportunity to think about the feedback.
PERSONAL RESPONSIBILITY
Whether an individual chooses to initiate change in their own behavior ultimately
is their responsibility. During the brief intervention, you should communicate
this principle clearly to the drinker and to the family members. Families
can help and support a person in their change efforts, and may serve as a
source of motivation for change, but the ultimate decision is an individual
one. You can communicate this principle through comments such as:
FAMILY INVOLVEMENT
The preceding sections have guided you in managing the family's reactions during
the brief intervention. Additional roles the family may play include:42
Providing Additional Feedback to the Drinker
This may include feedback about negative consequences resulting from drinking,
or objectionable behaviors observed when drinking; the results of previous
change attempts; or family members' subjective reactions to the drinking
or to the clinician's feedback. Encouraging the use of constructive communication
skills is key to successful family feedback. Suggest that they use "I" statements
rather than attacks, and expressions of care and concern rather than expressions
of blame or contempt.
Supporting the Drinker's Attempts to Change
This is a topic that may continue through future sessions, but which can be
introduced during the brief intervention. As the drinker decides upon a course
of action, you may ask the family to consider ways to support these actions.
Finding Ways to Support and Reinforce
Positive Change
Families might spend more time with the drinker when abstinent, express positive
reactions to changes in drinking (e.g., "I really enjoyed today), or provide
positive feedback through concrete actions (e.g., a heartfelt hug.)
Stating Specific Limits
Family members may have decided on limits about what they will tolerate, and
what they plan to do should the drinking continue unchanged. Knowledge about
such limits might have an important influence on the drinker's decision-making.
FOLLOW-UP
Although most descriptions of brief interventions stop here, the family therapist
who implements a brief drinking intervention usually has an on-going relationship
with the family, and will have the opportunity to follow-up beyond the initial
intervention.
If the drinker and family settle on a change strategy by the end of the brief intervention, you should continue to check in and monitor success and problems in future treatment sessions.
If the initial plan is not succeeding, you can discuss further options. A tone of collaboration and respect should characterize these later discussions as well. For example:
It is a myth that family members cannot influence a drinker to change.
Family members cannot make an individual stop drinking, but they can
change their own behavior in ways that will help the drinker recognize
that the drinking is problematic, and that change is desirable. In fact,
study findings support the effectiveness of such interventions.43
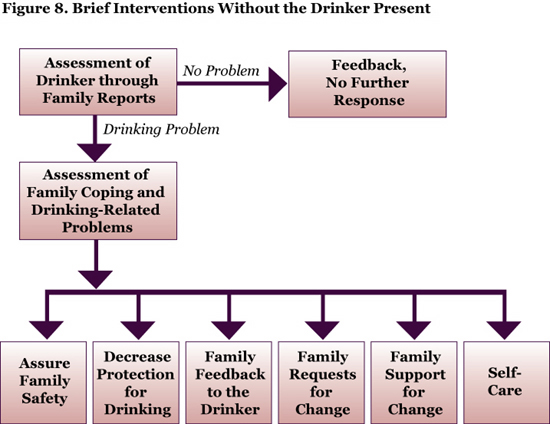 d d |
When family members are involved in treatment without the drinker, a careful assessment is required to determine whether the affected family members are dealing with a loved one who has a drinking problem. This initial assessment should be followed up with confirmatory feedback. Providing further assessment of family coping strategies and offering guidance in specific responses form the core of such interventions. Safety issues and other aspects of self-care must also be addressed, regardless of the drinker's behavior (See Assuring Family Safety).
Several aspects of brief interventions with the drinker not present are similar to those described previously for brief interventions with the drinker present. Others are unique to the situation where the drinker is not available to the therapist. Key elements include:
ASSESSMENT AND FEEDBACK ABOUT
THE DRINKER'S DRINKING
Family members often are uncertain about the seriousness of the drinking of
another family member. You can conduct an assessment similar to that described
for the drinker using the family member's report.
Ideally, you will be able to determine whether an alcohol problem is present or establish a diagnosis of alcohol abuse or dependence based on the family member's report, and also assess the quantity and frequency of drinking. After making this determination, you should give the family feedback, either to assure them that the drinking is not objectively a problem, or that it is problematic or a diagnosable disorder. If the drinking pattern is neither problematic nor diagnosable, then your intervention should focus on discussing the different attitudes and values about drinking in the family. If the drinking is problematic, a more detailed family intervention is needed.
ASSESSMENT OF FAMILY COPING STRATEGIES
How families cope with the drinking is an important area of assessment. Families
engage in a wide range of responses to drinking, including behaviors that
support or tolerate the drinking, confront or control the drinking, or attempt
to withdraw from the drinking or the drinker.
You can assess family coping through interviews as well as questionnaires. In an interview, ask questions such as:
There are several good questionnaires to assess family coping, including The Coping Questionnaire,44 the Significant-Other Behavior Questionnaire,45 the Spouse Enabling Inventory,46 and the Spouse Sobriety Influence Inventory.47
As with a drinker's assessment, an assessment of family coping should be approached in a spirit of inquiry by engaging the family in a discussion that reveals their perceptions about positive and negative actions, as well as their subjective feelings about interactions with the drinker. This assessment of family coping strategies sets the stage for suggested interventions.
ASSURING FAMILY SAFETY
Spouse and child abuse occur at elevated rates in families where one member
has an alcohol problem. You should conduct a specific assessment for the
presence of physical violence if there are drinking issues in the family.
Assessment should target specific aggressive behaviors, rather than global
questions such as, "Is there any violence in your home?" Specific
questions should be asked about behaviors such as throwing objects, grabbing
a family member roughly, slapping, pushing, hitting, or threatening harm.
The Conflict Tactics Scale can be used to conduct a more formalized assessment
of domestic violence. For more information on the
Conflict Tactics Scale, go to: www.unh.edu/frl/measure4.htm.
Additional questions about actual injuries also should be included in the assessment. The presence of weapons in the home, particularly guns, also should be noted.
If there is evidence of physical violence in the family, you must take steps to assure the safety of the family. Since some families may view such behavior as normal, it is essential that you make a clear, unambiguous statement about the need for safety and the unacceptability of being hit or otherwise hurt. Advising the family on other safety measures — such as keeping a bag packed, establishing a place to go should violence appear imminent, and understanding the role and limitations of restraining orders — also is appropriate. If there are guns or other weapons in the home, you should consider advising either their removal or a secure locking system to prevent a potentially violent family member from accessing the weapons.48 Further information about intimate partner violence and treatment can be found at www.cdc.gov/health/violence.htm and at the AMA Violence Prevention page at www.ama-assn.org/ama/pub/category/3242.html , which features the monograph titled Intimate Partner Violence: Case Studies in Disease Prevention and Health Promotion.
CHANGING FAMILY COPING
Once you have assured the basic safety of the family, you can begin to address
changes in family behavior that may help the drinker recognize his/her drinking
as problematic.
Changing Consequences of Drinking
It is common for family members to try to protect the drinker from the naturally
occurring negative consequences of drinking. They may assume the drinker's
responsibilities; cover for the drinker at work; provide comfort and reassurance
after a drinking binge; hide their feelings about the drinking; hide the
drinker's problems from family or friends, etc. Each of these actions may
be well intentioned, but the net effect is to shield the drinker from the
consequences of absences from work, the full impact of a hangover, or the
realization that a loved one is frightened or angry.
The drinker who has the opportunity to hear about such consequences gradually may realize that there is a large cost associated with drinking and may begin to consider change. You can help the family recognize the unintended adverse effects of protecting the drinker, guide them to reduce actions that protect the drinker, and help them recognize that there are certain actions that are necessary to preserve the family (such as paying bills), or the life of the drinker and others (such as not letting a person drive when intoxicated). Problem-solving, role-playing new responses during the treatment session, and giving specific homework assignments that involve practicing new behaviors are all excellent approaches to implementing these new behaviors.
Family Feedback to the Drinker
A second active intervention is providing direct feedback to the drinker. Families
may communicate in unproductive ways about drinking, for example, with nagging,
ridicule, and sarcasm. Your goal is to encourage them to use straightforward,
constructive communication techniques when giving their feedback. Remember
that feedback should be:
Family Requests for Change
Family members also can be guided to make specific, positive requests for change
from the drinker. Requests may be directed toward changes in the drinking
itself, toward behavior when drinking, or toward seeking assistance. You
can guide family members in articulating the changes they want and help them
practice how to make such requests. You should prepare the family by explaining
that the drinker does not always respond to such discussions or requests
with immediate acceptance. You should also help the family understand that
requests for change are part of the larger set of behavior changes described
in this section of the Guide.
Family Support for Change Efforts
Families also need to learn to support the drinker's efforts toward change.
They may resist providing support and encouragement, feeling that the drinker
is simply doing what he or she "should have done all along." Despite such
feelings, support for efforts to change is likely to increase them, while
ignoring such efforts or responding negatively likely will decrease attempts
at change. Family members can support change through verbal encouragement,
nonverbal gestures, or taking on family responsibilities to free up the drinker's
time for treatment or self-help meetings. You can work closely with the family
to identify supportive actions that are comfortable and acceptable to them.
Family Member Self-Care
Spouses with an actively drinking partner experience significant levels of
anxiety, depression, and psychophysiological complaints.49 Children
may have behavior problems, anxiety or depression, or eventually develop
alcohol or drug problems themselves. Thus, in addition to interventions to
attempt to influence the drinker, you should help family members learn how
to take care of their own needs.
Twelve-step organizations are one source of support that is specific for families of drinkers. Al-Anon is a self-help organization for adults affected by another's drinking; Alateen provides similar support for adolescents. Al-Anon and Alateen are widely available without cost to participants. The limited amount of research available on Al-Anon has demonstrated its effectiveness in helping to decrease distress among families affected by drinking.50 Specifically, Al-Anon is most effective as a source of support for the affected family member, and is not designed as a resource for motivating the drinking family member to change. Therefore, you should use this resource primarily as a source of support for affected family members.
Referral to a self-help group may serve as the only specialty referral in many locations, or it may be used to complement a formal treatment program. Several factors will guide the choice between these strategies:
 d d |
CHANGE THROUGH FAMILY-INVOLVED
TREATMENT
Two major approaches to family-based treatment for alcohol problems have been
developed and tested in controlled research — alcohol-focused behavioral
couples therapy (ABCT), and family systems approaches. ABCT is a structured
therapy based on cognitive-behavioral principles of behavior change.51 Major
components of ABCT include:
One empirical study has tested the effectiveness of family systems therapy to treat alcohol problems in adults. Family systems therapy views drinking as one aspect of the marital/family relationship and focuses on altering couple interactions that might be sustaining the drinking, as well as each partner's views of the meaning of the drinking. You may not require abstinence from drinking, but rather may prefer to help couples select and pursue a drinking goal of their own choosing. Both strategic and structural-family therapy techniques can be used to manage clients' ambivalence about change. Preliminary results suggest that such approaches are more effective than cognitive-behavioral approaches in retaining resistant and angry clients in therapy.54
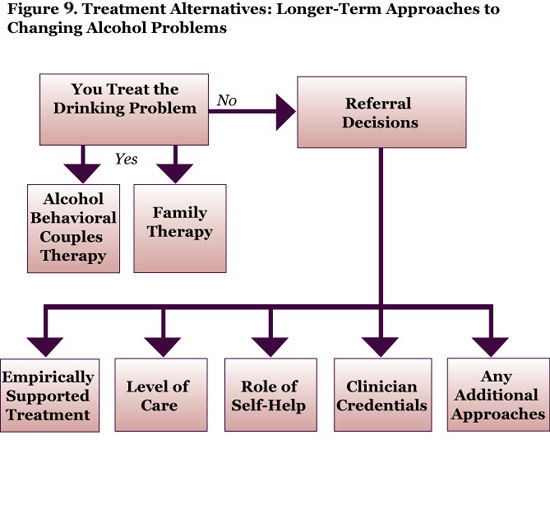
CHANGE THROUGH REFERRAL
A second long-term strategy is to refer clients to community-based services
for help with their drinking problems. Alcohol treatment services are provided
at different levels of care — inpatient, residential rehabilitative,
intensive outpatient, outpatient, or self-help.
There are two different approaches to selecting the level of care, and each has some support for its effectiveness. The first approach is stepped care, in which treatment is initiated at the least restrictive level possible for the client.55 It is usually a brief, outpatient intervention, and the intensity of treatment is increased only if the client does not respond to the initial intervention. The second approach, patient-treatment matching, is most fully articulated by the American Society of Addiction Medicine (ASAM) through their patient placement criteria (PPC).56
The PPC specify six dimensions to consider when selecting an initial level of care:
To effect a referral to the alcohol treatment system, you can obtain information about local treatment resources through your state alcohol and drug agency. Many states provide online treatment directories and/or have toll-free hotlines that provide information about treatment services.
In addition to knowledge about levels of care and credentials, you also should be aware of research knowledge about effective treatment approaches. Three treatment models have been studied extensively, and each has fairly consistent support for its effectiveness:57
SELF HELP GROUPS
Clinicians also should be aware of and familiar with self-help groups. Alcoholics
Anonymous (AA) provides a program of recovery based on twelve steps to recovery
that stress acceptance of drinking as a problem, willingness to seek help,
and personal and interpersonal change designed to enhance a spiritual approach
to life. AA is widely available, free of charge, and requires a desire to
stop drinking as the only "membership" requirement. Research studies have
found a significant though modest correlation between attending more AA meetings
and being abstinent, and an even stronger relationship between involvement
with AA (e.g., working the steps, reading AA literature, having a sponsor,
as well as going to meetings) and abstinence.
Other self-help groups are less widely available or researched, but provide alternative sources of self-help for clients who would like a self-help format but are unwilling to attend AA.58 Groups include Women for Sobriety, SMART Recovery, Secular Organizations for Recovery/LifeRing, Moderation Management, and culturally specific self help groups, such as Red Road for the American Indian population. Little research is available about the effectiveness of any of these organizations.
Drinking problems may range in severity, from differences in values and preferences about drinking that create family conflicts, to severe alcohol dependence. As a result, marriage and family therapists should screen all clients for possible drinking problems and complete additional assessments where appropriate. When determining whether to intervene and how to intervene, it is important to first consider the overall goals of family therapy and any safety concerns that may be involved. Brief interventions, either directly with the drinker or with concerned family members, can have a positive impact on alcohol problems.
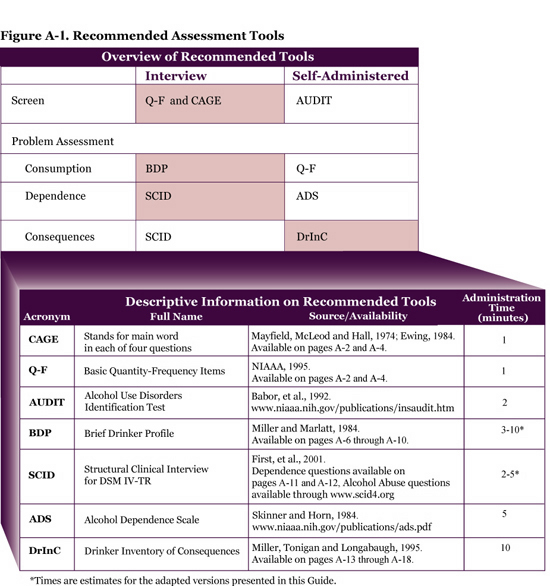
CLINICAL TOOLBOX FOR SCREENING AND ASSESSMENT
OF ALCOHOL PROBLEMS
The instruments and interview questions provided in this Clinical Toolbox will
enable you to conduct screening and assessments of alcohol problems in your
own practice. The figure below provides an overview of a few recommended tools
in both interview and self-administered formats. Selection of self-report or
interview formats will be determined by clinician skill and preference, as
well as client literacy.
The tools in the shaded boxes represent a complete protocol for screening
and problem assessment and are reproduced in this Appendix. The other
instruments are available from the sources indicated.
 d d |
TOOLS FOR SCREENING
Although we have selected the CAGE questions to use in the screening protocol
that follows, any of the screening instruments described earlier may be substituted
for the CAGE. If you plan to use self-administration rather than an interview
format, we suggest you use the Alcohol Use Disorders Identification Test
(AUDIT) rather than the CAGE, because it includes consumption questions with
standardized response options. If you determine that an interview is the
appropriate format for your screening protocol, we recommend the following
set of screening questions:
Basic Quantity-Frequency Questions (Self
Report)
CAGE Questions (Self Report)
| Interpreting Risk from the Screening
Questions An individual may be at risk for alcohol-related problems if alcohol consumption is:
One or more responses to the CAGE questions referring to the past year were positive. |
TOOLS FOR COLLATERAL SCREENING
Gathering "collateral" reports (e.g., a spouse reports on their partner's drinking)
may be useful in helping you identify potential alcohol problems in the family.
Furthermore, it is important to determine whether family members who are not
present for therapy may have an alcohol problem, particularly when the presenting
problem involves couple or family issues. The following general questions about
drinking and family life may be incorporated into any standard family intake:
Family/Relational Drinking Conflict Questions
(These questions, when asked, may be used to reference "anyone" in the family,
or may be asked specifically about the spouse.)
Basic Quantity-Frequency Questions (Family
Member Report)
CAGE Questions (Family Member Report)
See the box "Interpreting Risk from the Screening Questions" above to make decisions about further assessments.
| Remember: Answers to the screening questions and these interpretive guidelines may be used initially to help you gauge the potential for alcohol problems in the family. A diagnosis, however, should not be made based on these questions alone. If an individual or family "screens positive," suggesting indications of risk, further assessment is required to confirm the risk and to determine the nature, extent, and severity of the problem. |
Source: Adapted from,
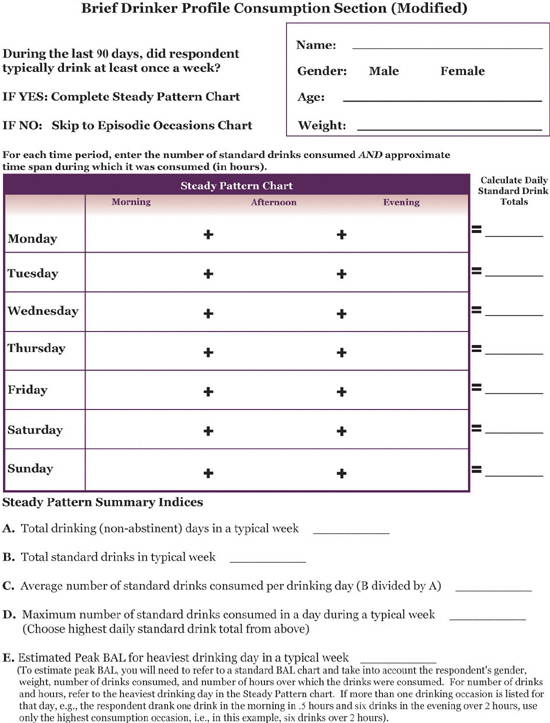
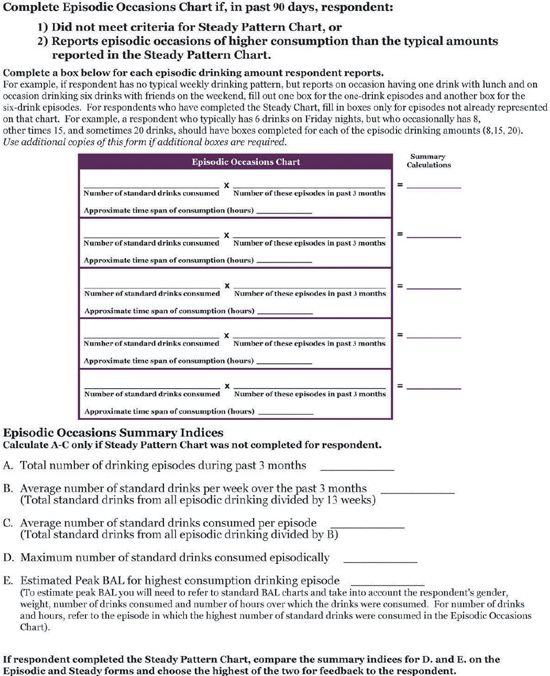
A TOOL FOR ASSESSING ALCOHOL
CONSUMPTION: THE BRIEF DRINKER PROFILE (MODIFIED)
Brief Quantity-Frequency (Q-F) questions, such as those described earlier (See
Basic Quantity-Frequency Questions on pages A-2 and A-4), may be used to
assess consumption patterns. However, the consumption section of the Brief
Drinker Profile is recommended because it yields more information on drinking
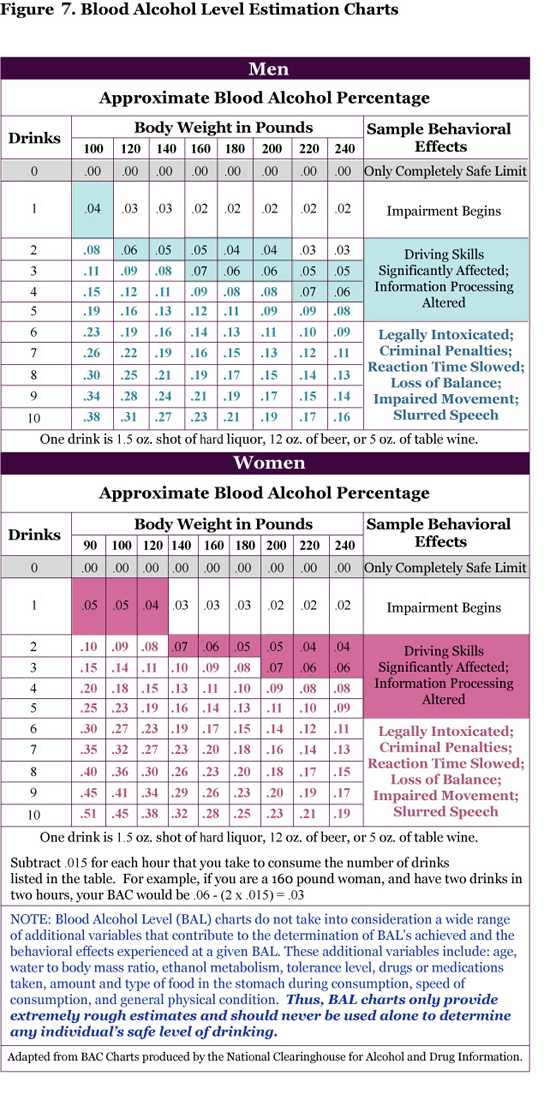
patterns, including information that will allow you to calculate peak BAL levels.
The information derived from the BDP should not only give you a more accurate
assessment of the client's consumption pattern, but also provide a range of
summary indices that can be used in your brief intervention feedback session
(See Feedback, page 27).
The modified version of the BDP presented here assesses:
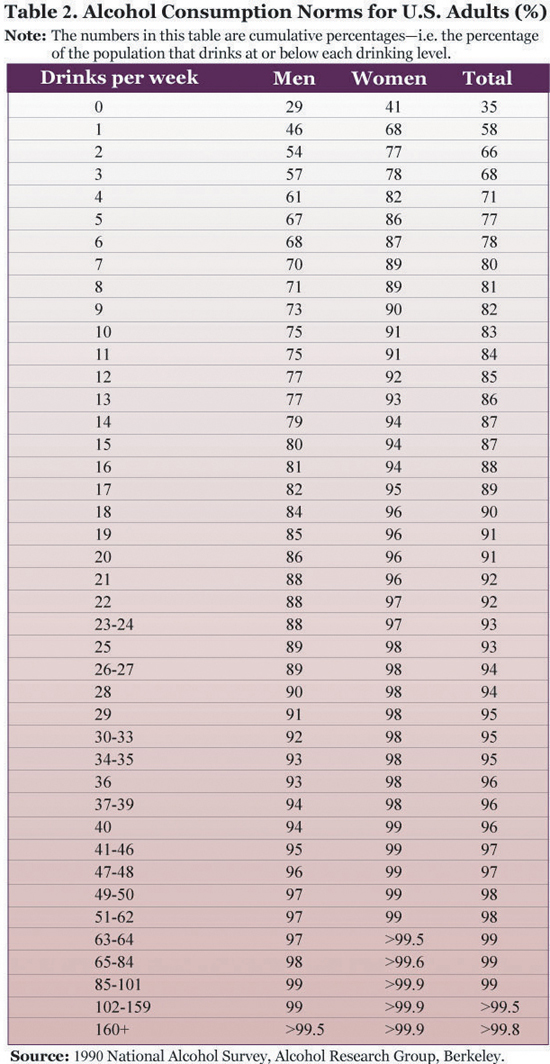
This consumption assessment uses the metric of standard drinks. Prior to conducting the BDP interview, you should familiarize yourself with the definition and equivalencies for a standard drink. A graphic portrayal of standard drink equivalencies is available in Appendix B. It is recommended that you reproduce this graphic and use it in consultation with the respondent during the interview to arrive at accurate standard drink estimates. To arrive at standard drink estimates, you should probe for the number of drinks consumed as well as the type of beverage and size of the drink, and then work with the respondent to arrive at the number of standard drinks consumed.
Although this interview protocol may also be conducted using a 30-day time frame, we use a 90-day (3-month) time frame in the protocol and attached forms to capture less frequent incidents of heavy drinking. To help the respondent accurately remember drinking occasions during the specified time frame, it is helpful to have a calendar available marked with holidays and other events that may provide "anchors" for the time frame.
You can introduce the assessment as follows:
Source: Adapted from Miller,
W.R., and Marlatt, G.A. (1984). Brief Drinker Profile. Odessa, FL: Psychological
Assessment Resources.
 d d |
 d d |
A TOOL FOR ASSESSING DEPENDENCE:
THE SCID ALCOHOL
DEPENDENCE QUESTIONS
The questions below are taken from the alcohol dependence section of the Structured
Clinical Interview for DSM-IV-TR Patient Edition (SCID-I/P). SCID questions
for use in the diagnosis of alcohol abuse, as well as a full version of the
SCID designed for clinical assessment of all Axis I disorders, are also available
(See www.scid4.org).
The SCID questions are designed to allow clinicians and researchers to systematically evaluate each of the seven indicators of dependence specified in the DSM-IV-TR diagnostic criteria. As noted in Figure 1 on page 2 of this Guide, the DSM-IV-TR Criteria for Alcohol Dependence involve finding three or more of the following in a 12-month period:
Since the SCID questions do not follow the ordering of the indicators in DSM-IV, we have indicated the relevant indicator for each question in the interview protocol below.
Dependence Assessment Interview Protocol
I'd like to ask you some questions about your drinking habits IN THE PAST
12 MONTHS.
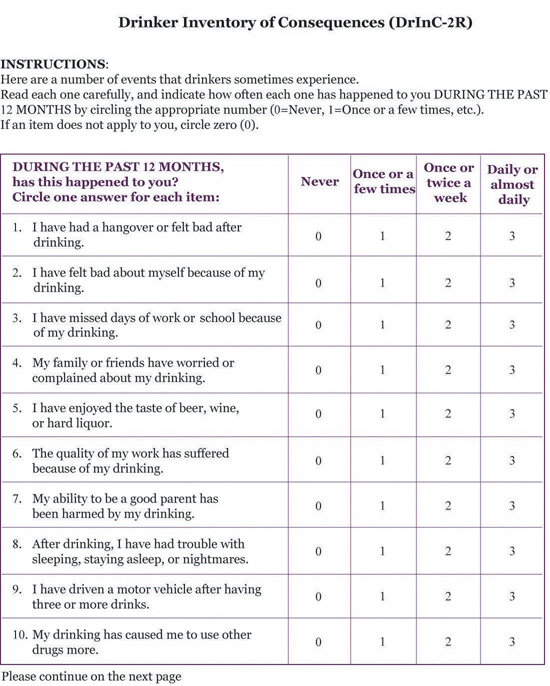
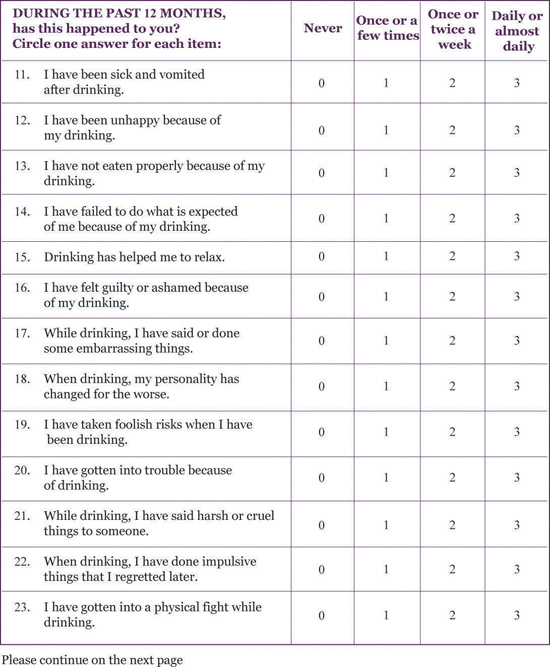
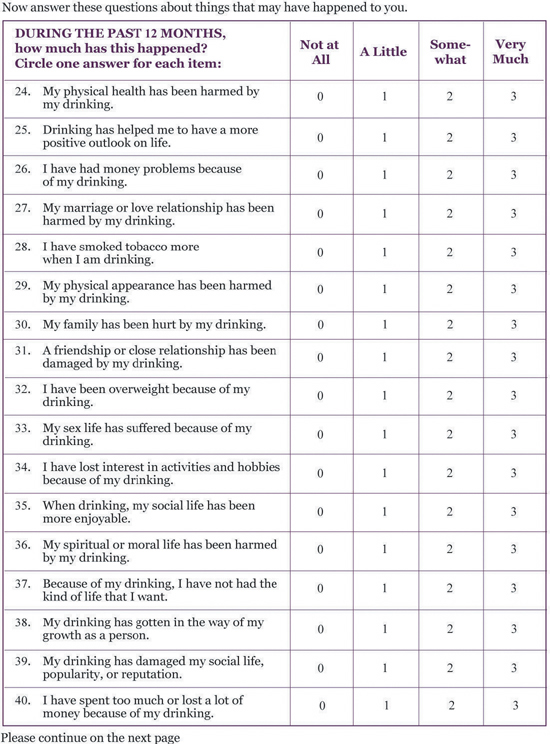
A TOOL FOR ASSESSING CONSEQUENCES:
DRINKER INVENTORY OF CONSEQUENCES
The Drinker Inventory of Consequences is a self-administered 50-item questionnaire
designed to measure adverse consequences of alcohol abuse in five areas: Interpersonal,
Physical, Social, Impulsive, and Intrapersonal. This scale has been adapted
to provide a 12-month measure of adverse consequences (Other versions of the
DrInC are available at http://casaa-0031.unm.edu/inst/inst.html).
Reproducible forms for self administration of the DrInC appear on the pages that follow.
Source: Adapted from Miller, W. R., Tonigan, J. S., and Longabaugh, R. (1995). The Drinker Inventory of Consequences (DrInC): An instrument for assessing adverse consequences of alcohol abuse. NIAAA Project MATCH Monograph Series, Vol. 4, U.S. Department of Health and Human Services, Bethesda, MD.
 d d |
 d d |
 d d |
 d d |
| d |
 d d |
MATERIALS FROM NIAAA
Assessing Alcohol Problems: A Guide
for Clinicians and Researchers - This handbook
reviews and recommends instruments and scales for assessing alcohol
problems to enable even those new to the field to understand the critical
issues involved in formal evaluation of alcoholism and alcohol treatment,
and to compare alternative measures. Handbook Series 5 due for release
in 2003.
Frequently Asked Questions Concerning Alcohol Abuse and Alcoholism - English version: NIH Publication No. 01-4735; Spanish version: NIH Publication No. 02-4735-S.
Alcoholism: Getting the Facts - A booklet that describes alcoholism and alcohol abuse and offers useful information on when and where to seek help. English version: NIH Publication No. 96-4153; Spanish version: NIH Publication No. 99-4153-S.
Alcohol: A Women's Health Issue - This 12-minute video describes the effects of alcohol on women's health at different life stages and includes first-person accounts of women of various ages and ethnic groups who are in recovery, with on-screen information on the prevalence and effects of alcohol problems. NIH Publication No. 02-5152.
Alcohol: What You Don't Know Can Harm You - A pamphlet that provides information on drinking and driving, alcohol-medication interactions, interpersonal problems, alcohol-related birth defects, long-term health problems, and current research issues. English version: NIH Publication No. 99-4323; Spanish version: NIH Publication No. 99-4323-S.
Drinking and Your Pregnancy - This booklet briefly conveys the lifelong medical and behavioral problems associated with Fetal Alcohol Syndrome and advises women not to drink during pregnancy. Revised 2001. English version: NIH Publication No. 96-4101; Spanish version: NIH Publication No. 97-4102.
How To Cut Down on Your Drinking - A pamphlet that presents tips for those who are acting on medical advice to reduce their alcohol consumption. English version: NIH Publication No. 96-3770; Spanish version: NIH Publication No. 96-3770-S.
Helping Patients with Alcohol Problems: A Health Practitioner's Guide - A guide on screening and brief interventions for primary care practitioners, physicians, physician's assistants, nurse practitioners and others who see patients for general health care. Second Edition due for release Spring 2003.
Alcohol Alerts - These 4-page bulletins provide timely information on alcohol research, prevention and treatment issues including: patient treatment matching, women, the workplace, alcohol and minorities, AIDS, co-occurring disorders, fetal alcohol exposure and the brain, aging, sleep, and more.
Alcohol Research & Health - Each issue of this quarterly, peer-reviewed journal contains review articles on a central topic related to alcohol research including issues such as violence, children of alcoholics, preventing alcohol problems, and alcohol and stress, to name just a few.
Interactions Between Alcohol and Various Classes of Medications - A laminated 8-1/2- by 11-inch desk chart listing drug classes, generic names, brand names, and types of interactions between alcohol and medications.
These publications are available in full text on NIAAA's Web site at: www.niaaa.nih.gov.
Print copies are available from:
NIAAA Publications Distribution Center
P.O. Box 10686, Rockville, MD 20849-0686
Phone: (301) 443-3860 or Fax: (301) 480-1726
RESOURCES FROM AAMFT
Family Therapy Resources -
This online resource provides information on alcohol dependence and
a wide range of other marriage and family therapy topics. AAMFT members
can view and print out complete magazine and journal articles for free
at: www.familytherapyresources.net.
Alcohol Problems Consumer Update - Consumers can find information about alcohol problems and a variety of other issues addressed by marriage and family therapists. Online versions can be found at: http://www.therapistlocator.net/.
Print copies are available from:
American Association for Marriage and
Family Therapy
112 South Alfred Street, Alexandria VA, 22314-3061
Phone: (703) 838-9808 or Fax: (703) 838-9805
How
to Intervene: What Programs Work? Evidence-Based Interventions
http://samhsa_search.samhsa.gov/
|
Model and promising resilience-enhancing and violence prevention programs
have been identified by several different organizations, both governmental
and nongovernmental. The following section describes the publications
that these organizations provide. It should be emphasized that not
all use the same standards of evidence-based criteria to judge the
soundness of the programs that are recommended. B. United States Department
of Justice, Preventing Crime: What Works, What Doesn't, What’s
Promising
The most recent lists of DOJ model and promising programs are updated
regularly at the University of Maryland Web site,
Forty-five research-based parenting and family intervention models
were selected by CSAP for grants to increase the capacity of communities
to deliver best practices in effective parenting and family programs
(see Exhibit III). Another resource for communities and schools is
Understanding Substance Abuse Prevention—Toward the 21st Century:
A Primer on
Effective Programs. This publication, as well as the most up-to-date
list of CSAP model programs, may be viewed at the Web site of the Substance
Abuse and Mental Health Services Administration, http://www.samhsa.gov/csap. D. National Association
of School Psychologists’ Exemplary Mental Health Programs:
School Psychologists as Mental Health Service Providers
A list of NASP-recommended programs may be obtained from the National Association of School Psychologists, Director of Professional Information and Communication, 4340 East West Highway, Suite 402, Bethesda, MD 20814. Phone (301) 657-0270. http://www.naspweb.org.
Each of these programs was required to meet rigorous selection criteria, including an experimental design, evidence of a statistically significant deterrent effect, replication in at least one additional site with experimental design and demonstrated effects, and evidence that the deterrent effect was sustained for at least one year posttreatment. According to Elliott, these high standards reflect “the level of confidence needed to build a violence prevention initiative, with the objective of allowing communities to implement these programs with the confidence of effectiveness in deterring violence, if implemented with integrity.” See Exhibit I for a list of CSPV model and promising programs. Additional information can also be obtained from the CSPV Web site, http://www.colorado.edu/cspv.
The guide lists programs that have demonstrated significant effects
on risk and protective factors in controlled studies or community trials
and some that have also shown positive effects on health and behavior
problems. G. Center for Mental
Health Services, Literature on the Development of Resilience
Detection/Treatment of Mental Illness
Alcohol and
Other Drug Abuse
Access to Mental Health/Health Services
Post-Intervention
Additional information may be obtained from the Suicide Prevention Advocacy
Network, 5034 Odin’s Way, Marietta, GA 30068. Phone (888) 649-1366.
http://www.spanusa.org. J. United States General
Accounting Office
|
1.Cost/Insurance
Treatment of substance abuse can be expensive. Some companies
cover these expenses and many managed care programs are now supporting treatment
for addiction. They are realizing that the cost, both human and financial, of
drug and alcohol dependency far exceeds the price of treatment. If cost is an
issue always check your local yellow pages for county and state programs, as
well as church programs or Salvation Army.
2.Inpatient
Treatment
This may be necessary if the denial system is firmly entrenched
and if detoxification is required. If an intervention (see ![]() The
Intervention Center for more on this technique) has been necessary, sometimes
inpatient rehabilitation is part of the treatment. If there are dangerous physical
concerns regarding detoxification, then an inpatient treatment will be essential.
Detox is considered to be the beginning of treatment, not the treatment itself. To detox and discharge is ineffective
and dangerous unless ongoing therapeutic and community support is arranged.
The
Intervention Center for more on this technique) has been necessary, sometimes
inpatient rehabilitation is part of the treatment. If there are dangerous physical
concerns regarding detoxification, then an inpatient treatment will be essential.
Detox is considered to be the beginning of treatment, not the treatment itself. To detox and discharge is ineffective
and dangerous unless ongoing therapeutic and community support is arranged.
3.The ACCEPT© Model
Developed by Phoenix Helm Simpson LMFTand Kate
Amatruda MFCC, this model involves:
4.Appropriate Twelve Step Programs
As should be clear at this
point we are great supporters of the Twelve Step Programs due to their long
term effectiveness, compassion and 24 hour a day 7 day a week availability.
The Step One in the Twelve Step Programs is "![]() We admitted we were powerless over alcohol - that our lives had become
unmanageable."
We admitted we were powerless over alcohol - that our lives had become
unmanageable." ![]() Narcotic
Anonymous states:
Narcotic
Anonymous states:
The core of the Narcotics Anonymous recovery program is a series of personal activities known as the Twelve Steps, adapted from Alcoholics Anonymous. These "steps" include admitting there is a problem, seeking help, self-appraisal, confidential self-disclosure, making amends where harm has been done, and working with other drug addicts who want to recover. Central to the program is an emphasis on what is referred to as a "spiritual awakening," emphasizing its practical value, not its philosophical or metaphysical import, which has posed very little difficulty in translating the program across cultural boundaries. Narcotics Anonymous itself is nonreligious and encourages each member to
cultivate an individual understanding, religious or not, of this "spiritual awakening."
There are however, many clients who will resist the AA approach, and part of the task of the compassionate therapist is to explore the resistance, as well as know what other options are available to the client.
5. Cognitive-Behavioral
Approach
While this model differs in key ways from the focus of this course,
it is important to know of its methodology. There is an on-line manual on the ![]() Treatment of Cocaine
Addiction by Kathleen Carroll, Ph.D. for the National Institute of Drug
Abuse. Focus is on assisting clients to recognize triggers and situations in
which they are most likely to use the drug of choice, avoid the triggers when
possible, and learn new ways to cope.
Treatment of Cocaine
Addiction by Kathleen Carroll, Ph.D. for the National Institute of Drug
Abuse. Focus is on assisting clients to recognize triggers and situations in
which they are most likely to use the drug of choice, avoid the triggers when
possible, and learn new ways to cope.
6. Community
Reinforcement Model
The National Institute of Health has an on-line
manual for treating cocaine addiction using ![]() community
reinforcement vouchers by Alan J. Budney, Ph.D. and Stephen T. Higgins Ph.D.
This is a 24 week
program focusing on drug avoidance skills, lifestyle changes and relationship
counseling combined with objective monitoring (urinalysis) and rewards in the
form of vouchers with the goal of abstinence. Therapists are encouraged to be
active, involoved and have a good understanding of behavioral modification techniques.
community
reinforcement vouchers by Alan J. Budney, Ph.D. and Stephen T. Higgins Ph.D.
This is a 24 week
program focusing on drug avoidance skills, lifestyle changes and relationship
counseling combined with objective monitoring (urinalysis) and rewards in the
form of vouchers with the goal of abstinence. Therapists are encouraged to be
active, involoved and have a good understanding of behavioral modification techniques.
http://www.nida.nih.gov/TXManuals/CRA/CRA1.html
ContentsForewordBackground
|
|
|||||||||||
|
|
||||||||||||
|
||||||||||||
7. The Role
of Medication
Medication has two roles in the treatment
of chemical dependency. The first is in treating target symptoms such
as detoxification,
cravings, and withdrawal. The second use of psychotropics is with dual
diagnosis populations, those with depression, schizophrenia, bipolar
disorder, ADD and
ADHD, anxiety disorder, etc. It is unfortunately beyond the scope of
this course to examine the use of psychotropics with people who are addicts.
8.Support/Education
Program for Family and Addict
Many in-patient programs and community agencies have low cost
or free series of lectures regarding the dynamics of addiction and codependence.
These are valuable for the addict, the family and the therapist. Education is
the the major tool for confronting denial and beginning recovery.
9.Resources
Please go now to ![]() NCADI
(The National Clearinghouse for Alcohol and Drug Information) for their phone
resource list, including hotlines, self-help groups and web site treatment
organizations.
For a treatment facility in your locale, try searching for SAMHSA's
National Directory of Drug Abuse and Alcoholism Treatment and Prevention Programs.
NCADI
(The National Clearinghouse for Alcohol and Drug Information) for their phone
resource list, including hotlines, self-help groups and web site treatment
organizations.
For a treatment facility in your locale, try searching for SAMHSA's
National Directory of Drug Abuse and Alcoholism Treatment and Prevention Programs.
888-777-3773
|
©
2000 - 2010 www.psychceu.com
all rights reserved. |